

Noninvasive ventilation in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis of randomized controlled trials
- PMID: 37217643
- PMCID: PMC10202054
- DOI: 10.1038/s41598-023-35323-0
Noninvasive ventilation in patients with acute hypoxemic respiratory failure: a systematic review and meta-analysis of randomized controlled trials
Abstract
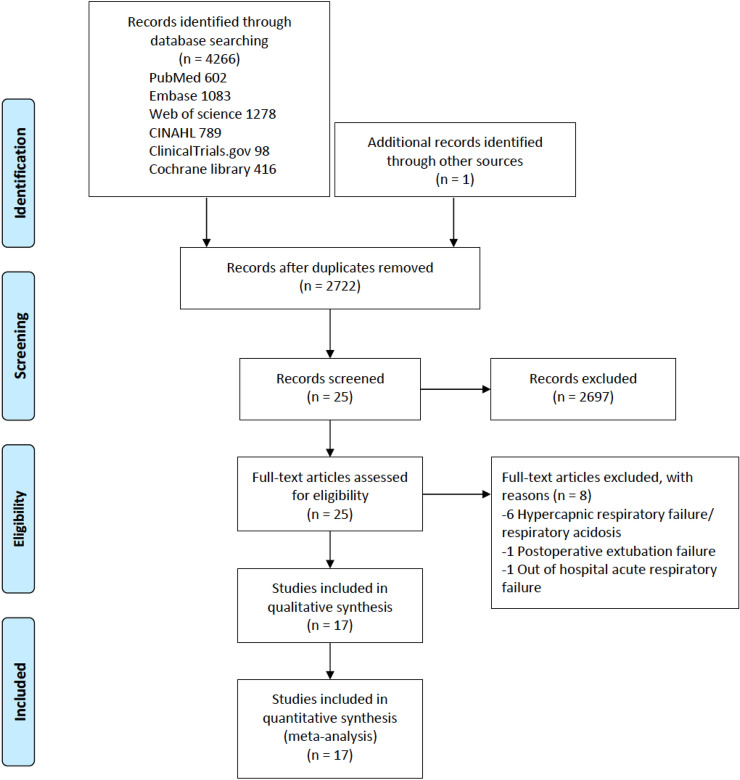
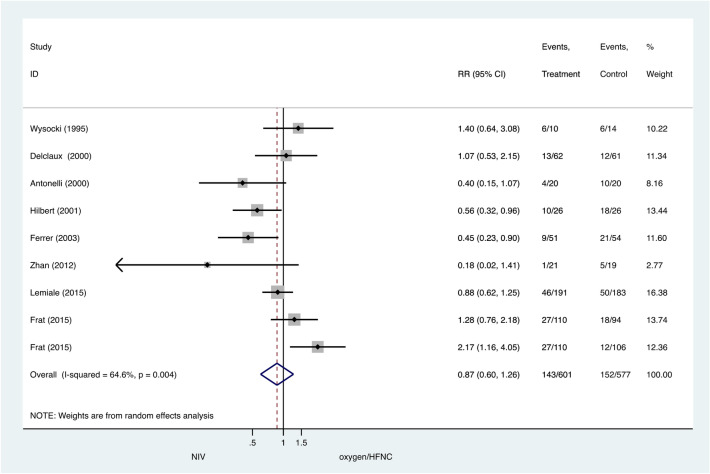
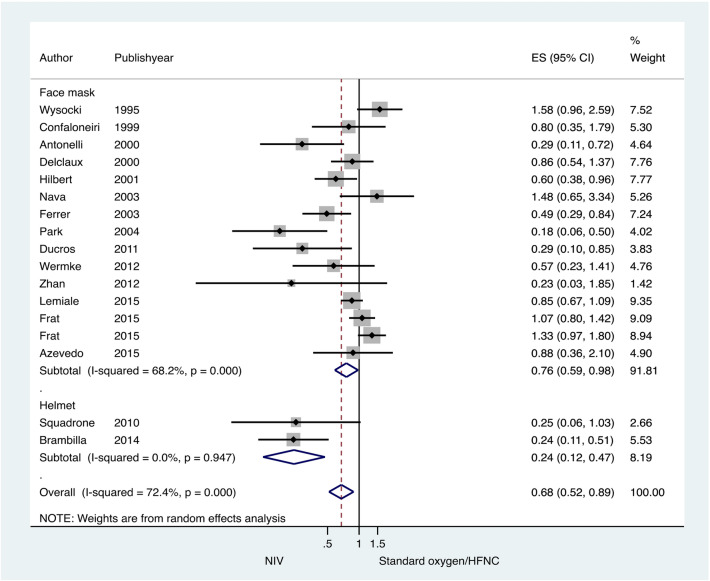
The clinical benefits of noninvasive ventilation (NIV) for patients with acute hypoxemic respiratory failure (AHRF) is still inconclusive. We aimed to evaluate the effect of NIV compared with conventional oxygen therapy (COT)/high-flow nasal cannula (HFNC) in this patient population. We searched for relevant studies from PubMed, Embase, Cochrane Library, ClinicalTrials.gov, CINHAL, Web of Science up to August 2019 for randomized controlled trials (RCTs) that compared NIV with COT/HFNC in AHRF. The primary outcome was the tracheal intubation rate. Secondary outcomes were intensive care unit (ICU) mortality, and hospital mortality. We applied the GRADE approach to grade the strength of the evidence. Seventeen RCTs that recruited 1738 patients were included in our meta-analysis. When comparing NIV versus COT/HFNC, the pooled risk ratio (RR) for the tracheal intubation rate was 0.68, 95% confidence interval (CI) 0.52-0.89, p = 0.005, I2 = 72.4%, low certainty of evidence. There were no significant differences in ICU mortality (pooled RR = 0.87, 95% CI 0.60-1.26), p = 0.45, I2 = 64.6%) and hospital mortality (pooled RR = 0.71, 95% CI 0.51-1.00, p = 0.05, I2 = 27.4%). Subgroup analysis revealed that NIV application with helmet was significantly associated with a lower intubation rate than NIV with face mask. NIV did not show a significant reduction in intubation rate compared to HFNC. In conclusion, NIV application in patients with medical illness and AHRF was associated with a lower risk of tracheal intubation compared to COT. NIV with helmet and HFNC are promising strategies to avoid tracheal intubation in this patient population and warrant further studies. NIV application had no effect on mortality.The study protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD42018087342).
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Kallet RH, Diaz JV. The physiologic effects of noninvasive ventilation. Respir. Care. 2009;54(1):102–115. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
