

Effect of core versus enhanced implementation strategies on adherence to a clinical pathway for managing anxiety and depression in cancer patients in routine care: a cluster randomised controlled trial
- PMID: 37217928
- PMCID: PMC10204284
- DOI: 10.1186/s13012-023-01269-0
Effect of core versus enhanced implementation strategies on adherence to a clinical pathway for managing anxiety and depression in cancer patients in routine care: a cluster randomised controlled trial
Abstract
Background: Optimal strategies to facilitate implementation of evidence-based clinical pathways are unclear. We evaluated two implementation strategies (Core versus Enhanced) to facilitate implementation of a clinical pathway for the management of anxiety and depression in cancer patients (the ADAPT CP).
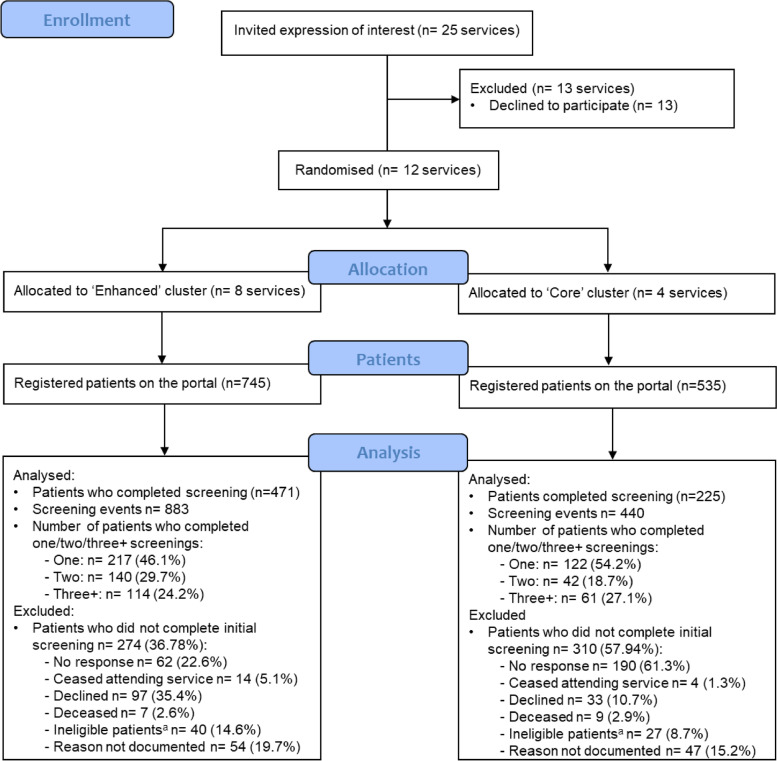
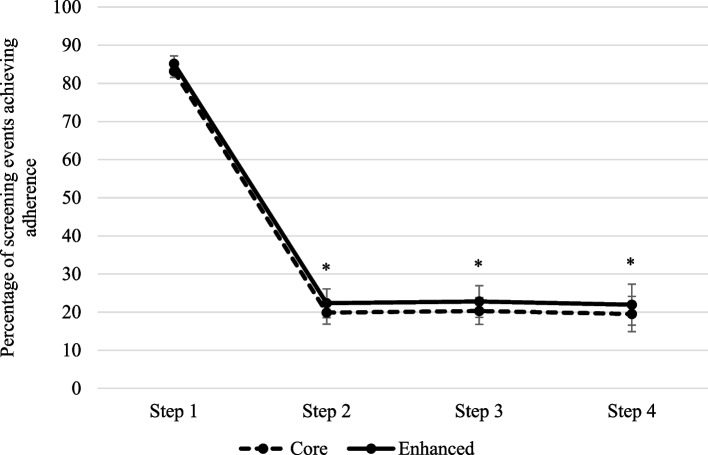
Methods: Twelve cancer services in NSW Australia were cluster randomised, stratified by service size, to the Core versus Enhanced implementation strategy. Each strategy was in place for 12 months, facilitating uptake of the ADAPT CP (the intervention being implemented). The Core strategy included a lead team with champions, staff training and awareness campaigns prior to implementation, plus access to feedback reports and telephone or online support during implementation. The Enhanced strategy included all Core supports plus monthly lead team meetings, and proactive, ongoing advice on managing barriers, staff training and awareness campaigns throughout implementation. All patients at participating sites were offered the ADAPT CP as part of routine care, and if agreeable, completed screening measures. They were allocated a severity step for anxiety/depression from one (minimal) to five (severe) and recommended management appropriate to their severity step. Multi-level mixed-effect regression analyses examined the effect of Core versus Enhanced implementation strategy on adherence to the ADAPT CP (binary primary outcome: adherent ≥ 70% of key ADAPT CP components achieved versus non-adherent < 70%), with continuous adherence as a secondary outcome. Interaction between study arm and anxiety/depression severity step was also explored.
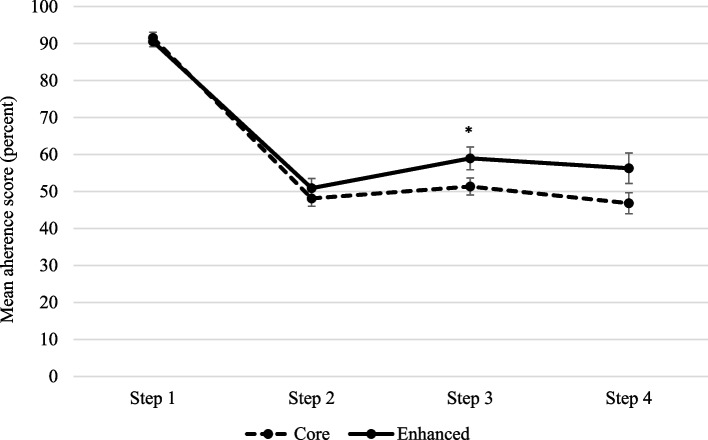
Results: Of 1280 registered patients, 696 (54%) completed at least one screening. As patients were encouraged to re-screen, there were in total 1323 screening events (883 in Core and 440 in Enhanced services). The main effect of implementation strategy on adherence was non-significant in both binary and continuous analyses. Anxiety/depression step was significant, with adherence being higher for step 1 than for other steps (p = 0.001, OR = 0.05, 95% CI 0.02-0.10). The interaction between study arm and anxiety/depression step was significant (p = 0.02) in the continuous adherence analysis only: adherence was significantly higher (by 7.6% points (95% CI 0.08-15.1%) for step 3 in the Enhanced arm (p = .048) and trending to significance for step 4.
Discussion: These results support ongoing implementation effort for the first year of implementation to ensure successful uptake of new clinical pathways in over-burdened clinical services.
Trial registration: ANZCTR Registration: ACTRN12617000411347 (Trial registered 22/03/2017; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372486&isReview=true ).
Keywords: Anxiety and depression management; Cluster randomised controlled trial; Implementation strategies.
© 2023. The Author(s).
Conflict of interest statement
The authors declare they have no competing interests.
Figures
References
-
- Queensland Health. Clinical Pathways. 2013; Available from: https://clinicalexcellence.qld.gov.au/resources/clinical-pathways.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
