

Evolocumab attenuate pericoronary adipose tissue density via reduction of lipoprotein(a) in type 2 diabetes mellitus: a serial follow-up CCTA study
- PMID: 37217967
- PMCID: PMC10204214
- DOI: 10.1186/s12933-023-01857-w
Evolocumab attenuate pericoronary adipose tissue density via reduction of lipoprotein(a) in type 2 diabetes mellitus: a serial follow-up CCTA study
Abstract
Background: Pericoronary adipose tissue (PCAT) density is a biomarker of vessel inflammation, which is supposed to be increased in patients with type 2 diabetes mellitus (T2DM). However, whether the coronary inflammation revealed by this novel index could be alleviated after evolocumab treatment in T2DM remains unknown.
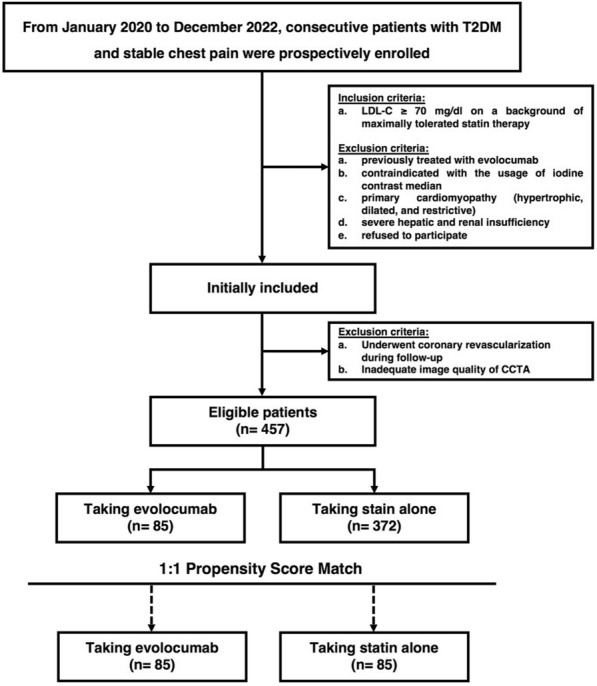
Methods: From January 2020 to December 2022, consecutive T2DM patients with low-density lipoprotein cholesterol ≥ 70 mg/dL on maximally tolerated statin and taking evolocumab were prospectively included. In addition, patients with T2DM who were taking statin alone were recruited as control group. The eligible patients underwent baseline and follow-up coronary CT angiography with an interval of 48-week. To render patients with evolocumab as comparable to those controls, a propensity-score matching design was used to select the matched pairs with a 1:1 ratio. Obstructive lesion was defined as the extent of coronary artery stenosis ≥ 50%; the numbers inside the brackets were interquartile ranges.
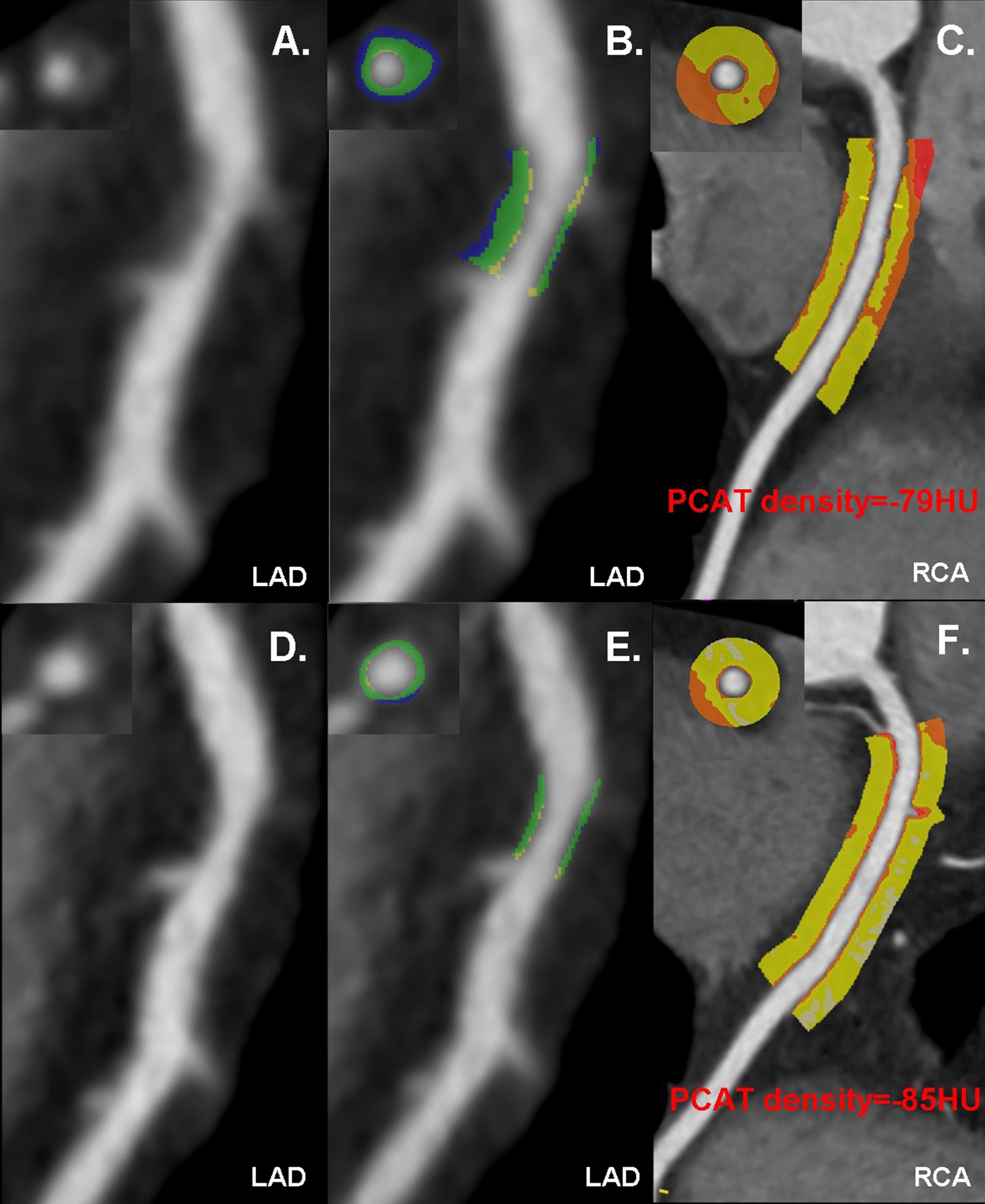
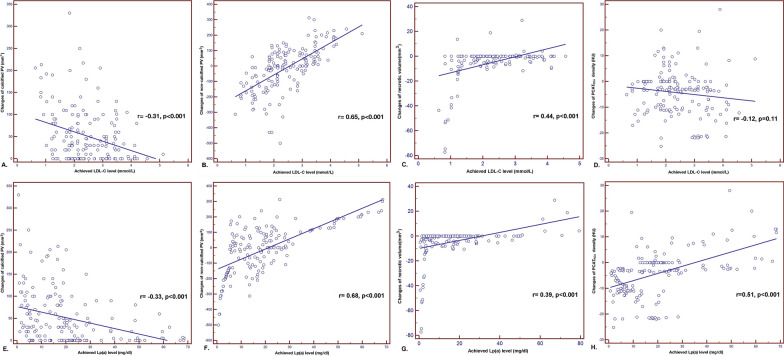
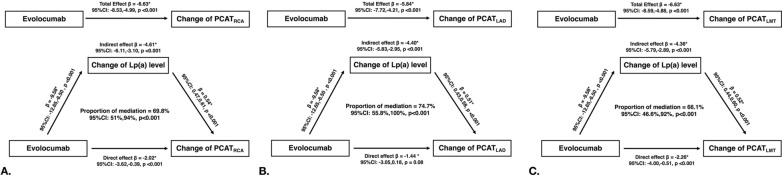
Results: A total of 170 T2DM patients with stable chest pain were included [(mean age 64 ± 10.6 [range 40-85] years; 131 men). Among those patients, 85 were in evolocumab group and 85 were in control group. During follow-up, low-density lipoprotein cholesterol (LDL-C) level (2.02 [1.26, 2.78] vs. 3.34 [2.53, 4.14], p < 0.001), and lipoprotein(a) (12.1 [5.6, 21.8] vs. 18.9 [13.2, 27.2], p = 0.002) were reduced after evolocumab treatment. The prevalence of obstructive lesions and high-risk plaque features were significantly decreased (p < 0.05 for all). Furthermore, the calcified plaque volume were significantly increased (188.3 [115.7, 361.0] vs. 129.3 [59.5, 238.3], p = 0.015), while the noncalcified plaque volume and necrotic volume were diminished (107.5 [40.6, 180.6] vs. 125.0 [65.3, 269.7], p = 0.038; 0 [0, 4.7] vs. 0 [0, 13.4], p < 0.001, respectively). In addition, PCAT density of right coronary artery was significantly attenuated in evolocumab group (- 85.0 [- 89.0, - 82.0] vs. - 79.0 [- 83.5, - 74.0], p < 0.001). The change in the calcified plaque volume inversely correlated with achieved LDL-C level (r = - 0.31, p < 0.001) and lipoprotein(a) level (r = - 0.33, p < 0.001). Both the changes of noncalcified plaque volume and necrotic volume were positively correlated with achieved LDL-C level and Lp(a) (p < 0.001 for all). However, the change of PCATRCA density only positively correlated with achieved lipoprotein(a) level (r = 0.51, p < 0.001). Causal mediation analysis revealed Lp(a) level mediated 69.8% (p < 0.001) for the relationship between evolocumab and changes of PCATRCA.
Conclusions: In patients with T2DM, evolocumab is an effective therapy to decrease noncalcified plaque volume necrotic volume, and increase calcified plaque volume. Furthermore, evolocumab could attenuate PCAT density, at least in part, via the reduction of lipoprotein(a).
Keywords: Coronary artery disease; Evolocumab; Lipoprotein(a); Multidetector computed tomography; Pericoronary adipose tissue.
© 2023. The Author(s).
Conflict of interest statement
Xin-Wei Tao is a current medical science liaison in Bayer Healthcare. Other authors do not have any competing interests to declare.
Figures
Similar articles
-
Pericoronary adipose tissue attenuation predicts compositional plaque changes: a 12-month longitudinal study in individuals with type 2 diabetes without symptoms or known coronary artery disease.Cardiovasc Diabetol. 2025 Mar 28;24(1):143. doi: 10.1186/s12933-025-02694-9. Cardiovasc Diabetol. 2025. PMID: 40155929 Free PMC article.
-
Lipoprotein(a) and Long-Term Plaque Progression, Low-Density Plaque, and Pericoronary Inflammation.JAMA Cardiol. 2024 Sep 1;9(9):826-834. doi: 10.1001/jamacardio.2024.1874. JAMA Cardiol. 2024. PMID: 39018040 Free PMC article.
-
Assessing the Impact of Long-Term High-Dose Statin Treatment on Pericoronary Inflammation and Plaque Distribution-A Comprehensive Coronary CTA Follow-Up Study.Int J Mol Sci. 2024 Jan 30;25(3):1700. doi: 10.3390/ijms25031700. Int J Mol Sci. 2024. PMID: 38338972 Free PMC article.
-
Additive effects of ezetimibe, evolocumab, and alirocumab on plaque burden and lipid content as assessed by intravascular ultrasound: A PRISMA-compliant meta-analysis.Medicine (Baltimore). 2022 Oct 14;101(41):e31199. doi: 10.1097/MD.0000000000031199. Medicine (Baltimore). 2022. PMID: 36254013 Free PMC article.
-
Imaging of the Pericoronary Adipose Tissue (PCAT) Using Cardiac Computed Tomography: Modern Clinical Implications.J Thorac Imaging. 2021 May 1;36(3):149-161. doi: 10.1097/RTI.0000000000000583. J Thorac Imaging. 2021. PMID: 33875629 Review.
Cited by
-
Pericoronary adipose tissue attenuation predicts compositional plaque changes: a 12-month longitudinal study in individuals with type 2 diabetes without symptoms or known coronary artery disease.Cardiovasc Diabetol. 2025 Mar 28;24(1):143. doi: 10.1186/s12933-025-02694-9. Cardiovasc Diabetol. 2025. PMID: 40155929 Free PMC article.
-
Coronary inflammation and atherosclerosis by CCTA in young adults (aged 18-45).Am J Prev Cardiol. 2025 May 24;22:101010. doi: 10.1016/j.ajpc.2025.101010. eCollection 2025 Jun. Am J Prev Cardiol. 2025. PMID: 40534630 Free PMC article.
-
PCSK9i and atherosclerotic plaque regression assessed by coronary computed tomography angiography: a meta-analysis.Clin Res Cardiol. 2025 May 19. doi: 10.1007/s00392-025-02672-x. Online ahead of print. Clin Res Cardiol. 2025. PMID: 40387889 No abstract available.
-
Computed tomography-based assessment of pericoronary adipose tissue in cardiovascular diseases: Diagnostic and prognostic implications.World J Radiol. 2025 Jun 28;17(6):107281. doi: 10.4329/wjr.v17.i6.107281. World J Radiol. 2025. PMID: 40606053 Free PMC article. Review.
-
Association between metformin treatment and coronary artery inflammation based on pericoronary adipose tissue attenuation in type 2 diabetes mellitus patients.J Clin Hypertens (Greenwich). 2024 Apr;26(4):330-337. doi: 10.1111/jch.14777. Epub 2024 Mar 2. J Clin Hypertens (Greenwich). 2024. PMID: 38430483 Free PMC article.
References
-
- Narayan KM, Boyle JP, Geiss LS, Saaddine JB, Thompson TJ. Impact of recent increase in incidence on future diabetes burden: US, 2005–2050. Diabetes Care. 2006;29(9):2114–6. - PubMed
-
- Malmberg K, Yusuf S, Gerstein HC, Brown J, Zhao F, Hunt D, Piegas L, Calvin J, Keltai M, Budaj A. Impact of diabetes on long-term prognosis in patients with unstable angina and non-Q-wave myocardial infarction: results of the OASIS (Organization to Assess Strategies for Ischemic Syndromes) Registry. Circulation. 2000;102(9):1014–1019. doi: 10.1161/01.CIR.102.9.1014. - DOI - PubMed
-
- Mak KH, Moliterno DJ, Granger CB, Miller DP, White HD, Wilcox RG, Califf RM, Topol EJ. Influence of diabetes mellitus on clinical outcome in the thrombolytic era of acute myocardial infarction. GUSTO-I Investigators. Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries. J Am Coll Cardiol. 1997;30(1):171–9. - PubMed
-
- McGill HC, Jr, McMahan CA, Malcom GT, Oalmann MC, Strong JP. Relation of glycohemoglobin and adiposity to atherosclerosis in youth. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. Arterioscl Thrombosis Vasc Biol. 1995;15(4):431–40. - PubMed
-
- Ray A, Huisman MV, Tamsma JT, van Asten J, Bingen BO, Broeders EA, Hoogeveen ES, van Hout F, Kwee VA, Laman B, et al. The role of inflammation on atherosclerosis, intermediate and clinical cardiovascular endpoints in type 2 diabetes mellitus. Eur J Intern Med. 2009;20(3):253–260. doi: 10.1016/j.ejim.2008.07.008. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
