

Cardiorespiratory Monitoring Data to Predict Respiratory Outcomes in Extremely Preterm Infants
- PMID: 37219236
- PMCID: PMC10870840
- DOI: 10.1164/rccm.202210-1971OC
Cardiorespiratory Monitoring Data to Predict Respiratory Outcomes in Extremely Preterm Infants
Abstract
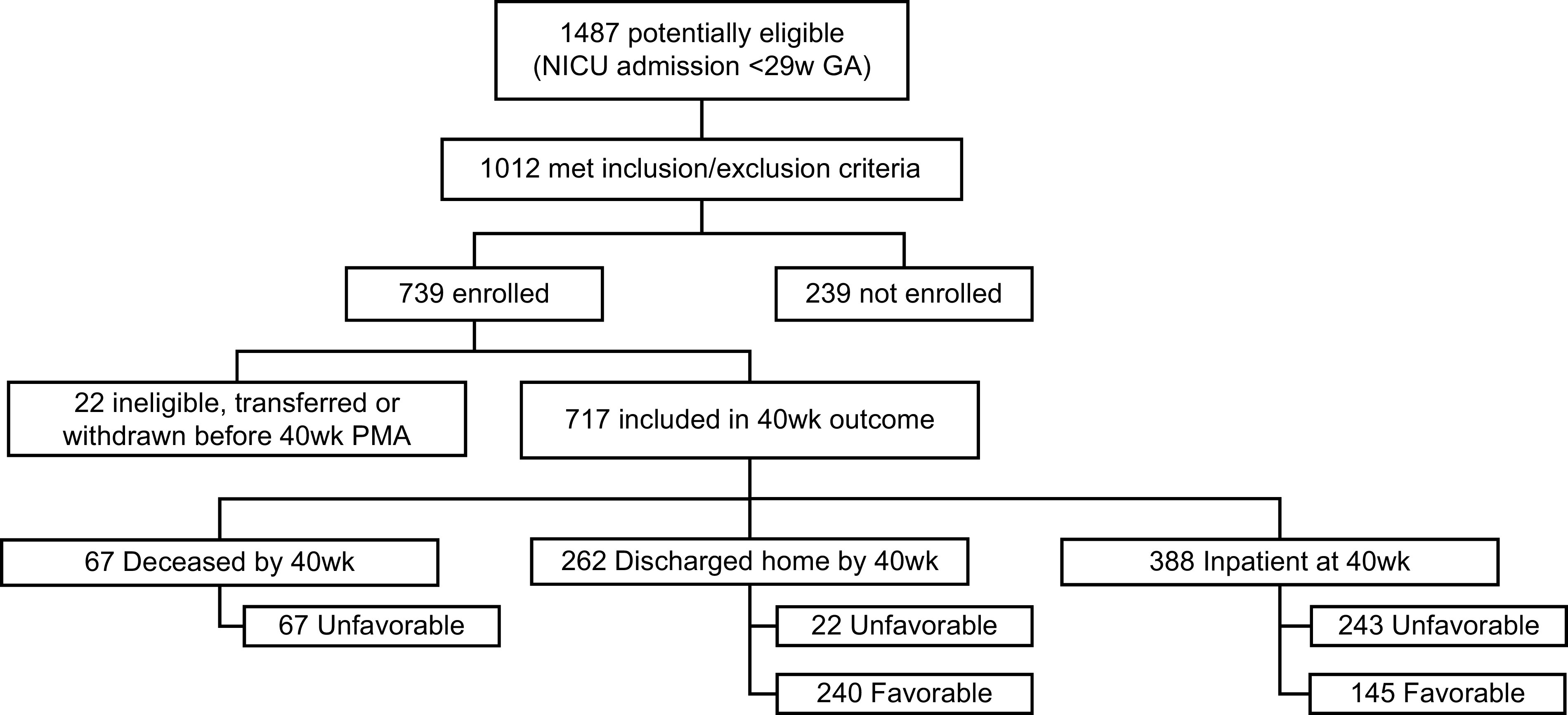
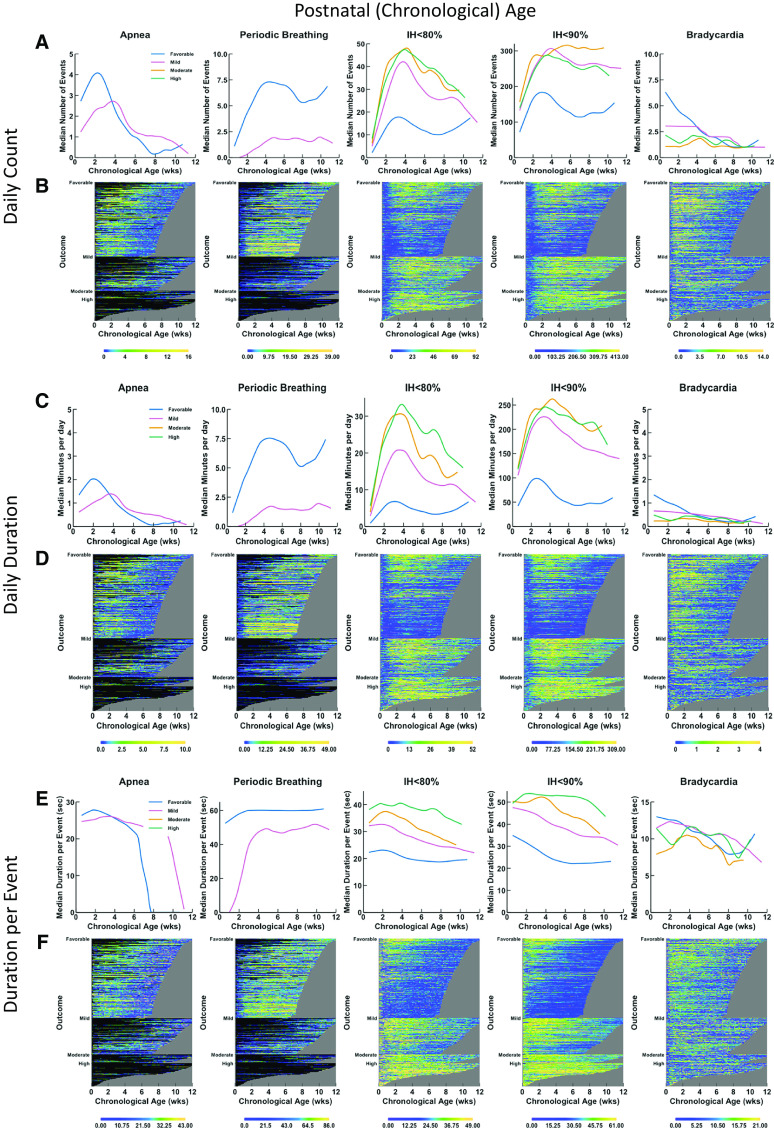
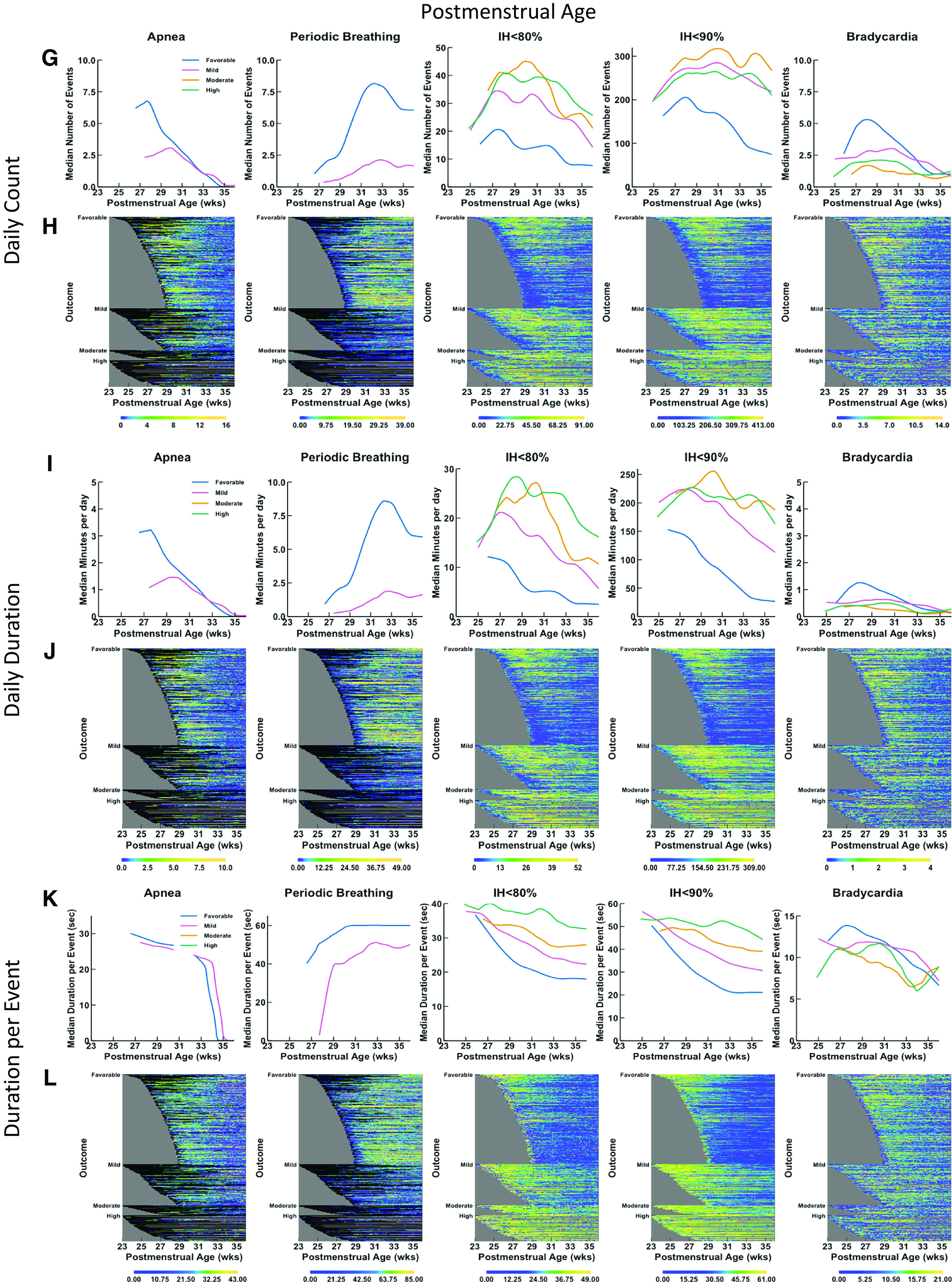
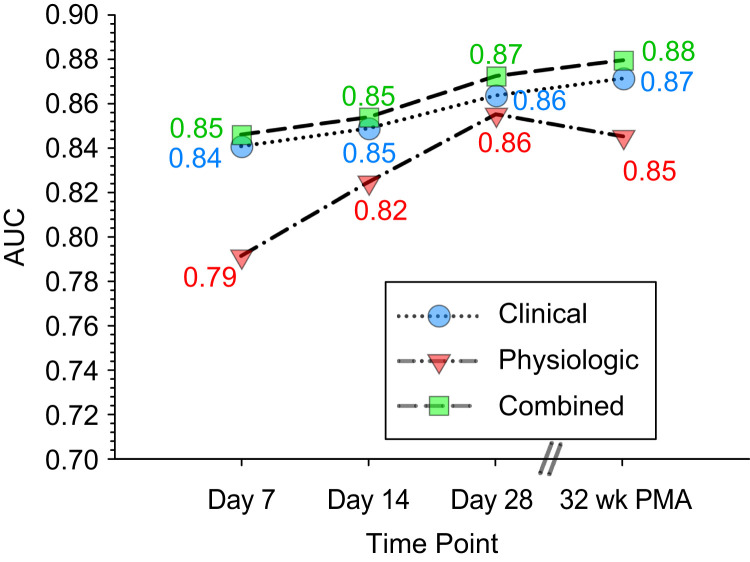
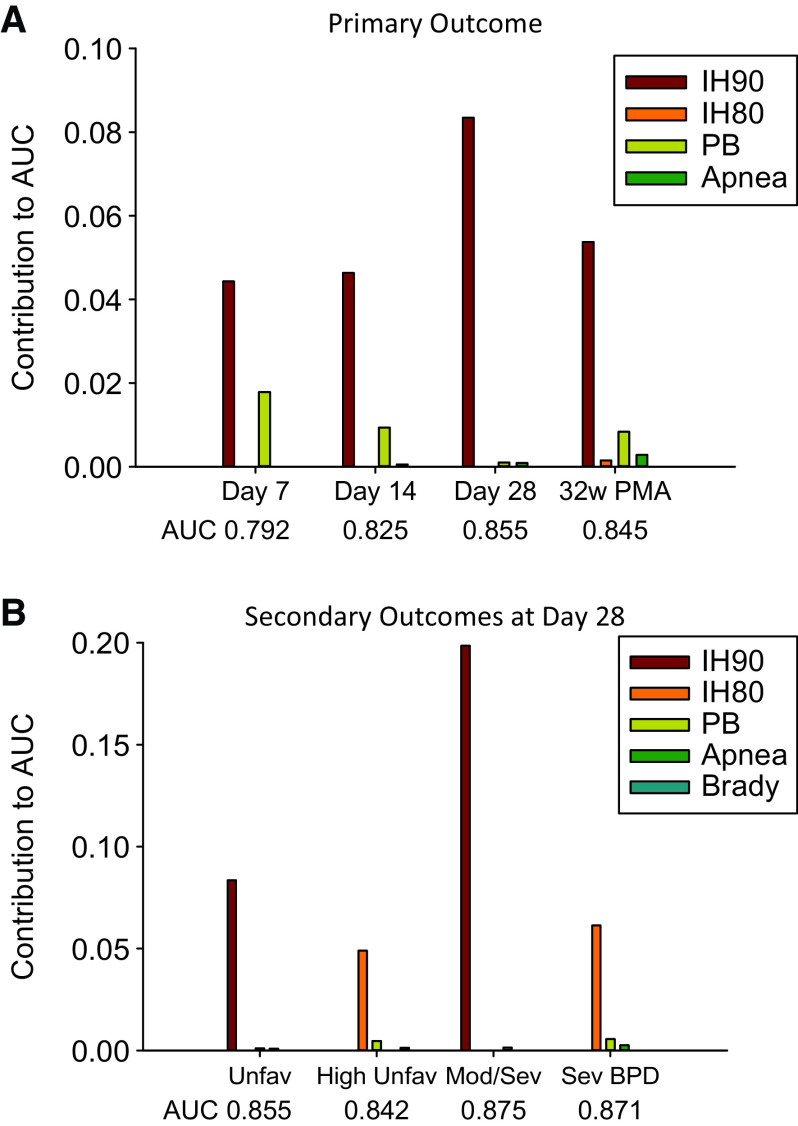
Rationale: Immature control of breathing is associated with apnea, periodic breathing, intermittent hypoxemia, and bradycardia in extremely preterm infants. However, it is not clear if such events independently predict worse respiratory outcome. Objectives: To determine if analysis of cardiorespiratory monitoring data can predict unfavorable respiratory outcomes at 40 weeks postmenstrual age (PMA) and other outcomes, such as bronchopulmonary dysplasia at 36 weeks PMA. Methods: The Prematurity-related Ventilatory Control (Pre-Vent) study was an observational multicenter prospective cohort study including infants born at <29 weeks of gestation with continuous cardiorespiratory monitoring. The primary outcome was either "favorable" (alive and previously discharged or inpatient and off respiratory medications/O2/support at 40 wk PMA) or "unfavorable" (either deceased or inpatient/previously discharged on respiratory medications/O2/support at 40 wk PMA). Measurements and Main Results: A total of 717 infants were evaluated (median birth weight, 850 g; gestation, 26.4 wk), 53.7% of whom had a favorable outcome and 46.3% of whom had an unfavorable outcome. Physiologic data predicted unfavorable outcome, with accuracy improving with advancing age (area under the curve, 0.79 at Day 7, 0.85 at Day 28 and 32 wk PMA). The physiologic variable that contributed most to prediction was intermittent hypoxemia with oxygen saturation as measured by pulse oximetry <90%. Models with clinical data alone or combining physiologic and clinical data also had good accuracy, with areas under the curve of 0.84-0.85 at Days 7 and 14 and 0.86-0.88 at Day 28 and 32 weeks PMA. Intermittent hypoxemia with oxygen saturation as measured by pulse oximetry <80% was the major physiologic predictor of severe bronchopulmonary dysplasia and death or mechanical ventilation at 40 weeks PMA. Conclusions: Physiologic data are independently associated with unfavorable respiratory outcome in extremely preterm infants.
Keywords: apnea; bronchopulmonary dysplasia; extremely premature infant; heart rate; intermittent hypoxemia; predictive value of tests.
Figures
Comment in
-
Predicting Pulmonary Outcomes in Extremely Preterm Infants from Recordings of Cardiorespiratory Data: A Question of Chicken and Egg.Am J Respir Crit Care Med. 2023 Jul 1;208(1):11-12. doi: 10.1164/rccm.202305-0809ED. Am J Respir Crit Care Med. 2023. PMID: 37219238 Free PMC article. No abstract available.
References
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet . 2015;385:430–440. - PubMed
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet . 2012;379:2162–2172. - PubMed
-
- Henderson-Smart DJ. The effect of gestational age on the incidence and duration of recurrent apnoea in newborn babies. Aust Paediatr J . 1981;17:273–276. - PubMed
-
- Di Fiore JM, Martin RJ, Gauda EB. Apnea of prematurity—perfect storm. Respir Physiol Neurobiol . 2013;189:213–222. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
