

Respiratory therapies for Amyotrophic Lateral Sclerosis: A state of the art review
- PMID: 37219417
- PMCID: PMC10214054
- DOI: 10.1177/14799731231175915
Respiratory therapies for Amyotrophic Lateral Sclerosis: A state of the art review
Abstract
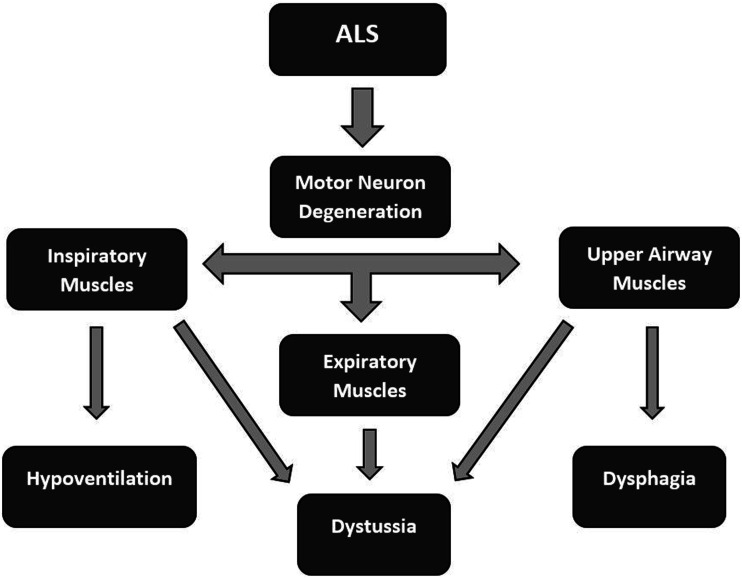
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative condition noteworthy for upper and lower motor neuron death. Involvement of respiratory motor neuron pools leads to progressive pathology. These impairments include decreases in neural activation and muscle coordination, progressive airway obstruction, weakened airway defenses, restrictive lung disease, increased risk of pulmonary infections, and weakness and atrophy of respiratory muscles. These neural, airway, pulmonary, and neuromuscular changes deteriorate integrated respiratory-related functions including sleep, cough, swallowing, and breathing. Ultimately, respiratory complications account for a large portion of morbidity and mortality in ALS. This state-of-the-art review highlights applications of respiratory therapies for ALS, including lung volume recruitment, mechanical insufflation-exsufflation, non-invasive ventilation, and respiratory strength training. Therapeutic acute intermittent hypoxia, an emerging therapeutic tool for inducing respiratory plasticity will also be introduced. A focus on emerging evidence and future work underscores the common goal to continue to improve survival for patients living with ALS.
Keywords: Amyotrophic lateral sclerosis; airway clearance; respiratory muscles; respiratory therapy; sleep disordered breathing; ventilation.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research,authorship, and/or publication of this article.
Figures


Similar articles
-
Combined Effects of Lung Volume Recruitment Training and Mechanical Insufflation-Exsufflation in a Patient With Advanced Amyotrophic Lateral Sclerosis Receiving Long-Term Mechanical Ventilation: A Case Report.Cureus. 2025 May 9;17(5):e83823. doi: 10.7759/cureus.83823. eCollection 2025 May. Cureus. 2025. PMID: 40491620 Free PMC article.
-
Airway Clearance Strategies and Secretion Management in Amyotrophic Lateral Sclerosis.Respir Care. 2024 Jan 24;69(2):227-237. doi: 10.4187/respcare.11215. Respir Care. 2024. PMID: 37816542 Free PMC article. Review.
-
Acute intermittent hypoxia and respiratory muscle recruitment in people with amyotrophic lateral sclerosis: A preliminary study.Exp Neurol. 2022 Jan;347:113890. doi: 10.1016/j.expneurol.2021.113890. Epub 2021 Oct 6. Exp Neurol. 2022. PMID: 34624328 Free PMC article. Clinical Trial.
-
Respiratory Failure in Amyotrophic Lateral Sclerosis.Chest. 2019 Feb;155(2):401-408. doi: 10.1016/j.chest.2018.06.035. Epub 2018 Jul 7. Chest. 2019. PMID: 29990478 Review.
-
Laryngeal response patterns influence the efficacy of mechanical assisted cough in amyotrophic lateral sclerosis.Thorax. 2017 Mar;72(3):221-229. doi: 10.1136/thoraxjnl-2015-207555. Epub 2016 May 12. Thorax. 2017. PMID: 27174631 Free PMC article.
Cited by
-
The Spatiotemporal Expression of SOCS3 in the Brainstem and Spinal Cord of Amyotrophic Lateral Sclerosis Mice.Brain Sci. 2024 May 31;14(6):564. doi: 10.3390/brainsci14060564. Brain Sci. 2024. PMID: 38928564 Free PMC article.
-
The role of ALDH2 rs671 polymorphism and C-reactive protein in the phenotypes of male ALS patients.Front Neurosci. 2024 Sep 3;18:1397991. doi: 10.3389/fnins.2024.1397991. eCollection 2024. Front Neurosci. 2024. PMID: 39290715 Free PMC article.
-
Long-term mechanical ventilation: State of the evidence and future directions.Chron Respir Dis. 2023 Jan-Dec;20:14799731231199764. doi: 10.1177/14799731231199764. Chron Respir Dis. 2023. PMID: 37649451 Free PMC article. No abstract available.
-
Analysis of Respiratory Muscle Strength Training in Amyotrophic Lateral Sclerosis (ALS) Patients: A Systematic Review.Cureus. 2025 Feb 12;17(2):e78903. doi: 10.7759/cureus.78903. eCollection 2025 Feb. Cureus. 2025. PMID: 40091916 Free PMC article. Review.
-
Hypotussic cough in persons with dysphagia: biobehavioral interventions and pathways to clinical implementation.Front Rehabil Sci. 2024 Jun 12;5:1394110. doi: 10.3389/fresc.2024.1394110. eCollection 2024. Front Rehabil Sci. 2024. PMID: 38933659 Free PMC article. Review.
References
-
- Brown RH, Al-Chalabi A. Amyotrophic lateral sclerosis. N Engl J Med 2017; 377: 1602–2172. - PubMed
-
- Andrews JA, Cudkowicz ME, Hardiman O, et al.VITALITY-ALS, a phase III trial of tirasemtiv, a selective fast skeletal muscle troponin activator, as a potential treatment for patients with amyotrophic lateral sclerosis: study design and baseline characteristics. Amyotroph Lateral Scler Frontotemporal Degener 2018; 19: 259–266. - PubMed
-
- Bruneteau G, Simonet T, Bauché S, et al.Muscle histone deacetylase 4 upregulation in amyotrophic lateral sclerosis: potential role in reinnervation ability and disease progression. Brain 2013; 136: 2359–2368. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
