

Prenatal Substance Exposure and Neonatal Abstinence Syndrome: State Estimates from the 2016-2020 Transformed Medicaid Statistical Information System
- PMID: 37219692
- PMCID: PMC10204012
- DOI: 10.1007/s10995-023-03670-z
Prenatal Substance Exposure and Neonatal Abstinence Syndrome: State Estimates from the 2016-2020 Transformed Medicaid Statistical Information System
Erratum in
-
Correction: Prenatal Substance Exposure and Neonatal Abstinence Syndrome: State Estimates from the 2016-2020 Transformed Medicaid Statistical Information System.Matern Child Health J. 2024 Mar;28(3):597. doi: 10.1007/s10995-023-03763-9. Matern Child Health J. 2024. PMID: 37460912 Free PMC article. No abstract available.
Abstract
Introduction: Estimating Neonatal Abstinence Syndrome (NAS) and prenatal substance exposure rates in Medicaid can help target program efforts to improve access to services.
Methods: The data for this study was extracted from the 2016-2020 Transformed Medicaid Statistical Information System (T-MSIS) Analytic Files (TAF) Research Identifiable Files (RIF) and included infants born between January 1, 2016 and December 31, 2020 with a either a NAS diagnosis or prenatal substance exposure.
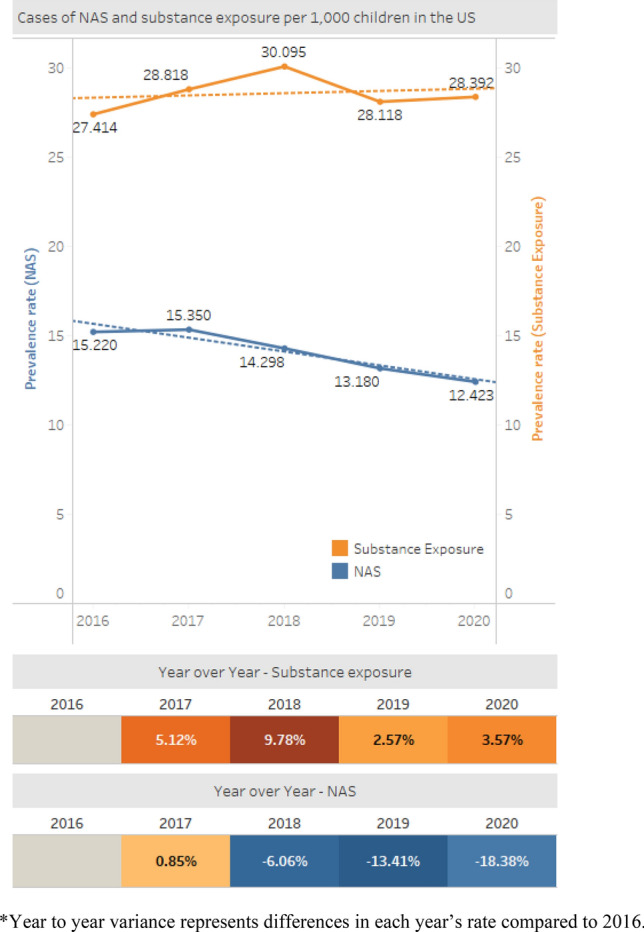
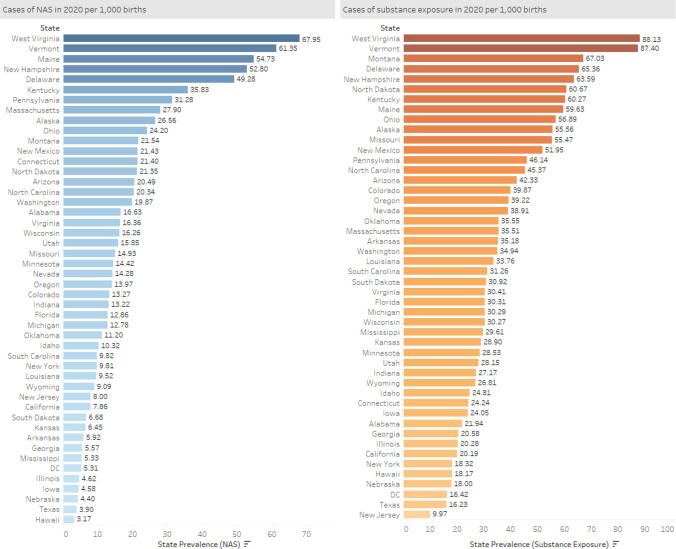
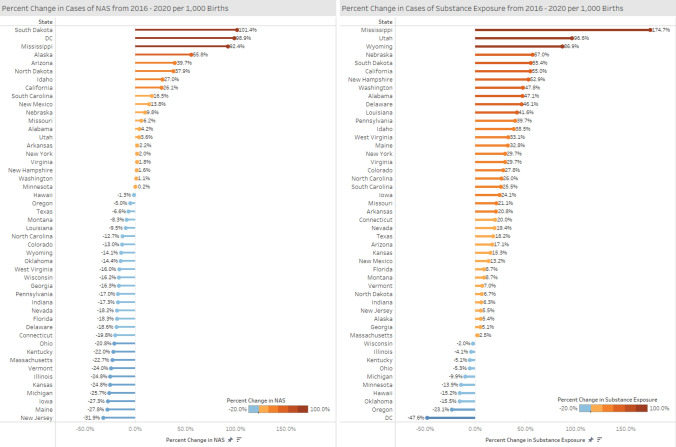
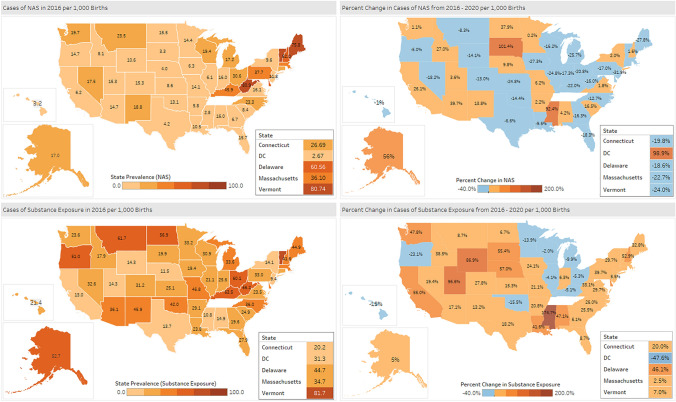
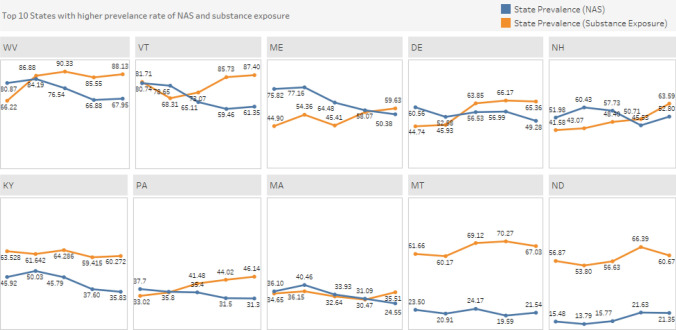
Results: Between 2016 and 2020, the estimated national rate of NAS experienced a 18% decline, while the estimated national rate of prenatal substance exposure experienced a 3.6% increase. At the state level in 2020, the NAS rate ranged from 3.2 per 1000 births (Hawaii) to 68.0 per 1000 births (West Virginia). Between 2016 and 2020, 28 states experienced a decline in NAS births and 20 states had an increase in NAS rates. In 2020, the lowest prenatal substance exposure rate was observed in New Jersey (9.9 per 1000 births) and the highest in West Virginia (88.1 per 1000 births). Between 2016 and 2020, 38 states experienced an increase in the rate of prenatal substance exposure and 10 states experienced a decline.
Discussion: Estimated rate of NAS has declined nationally, but rate of prenatal substance exposure has increased, with considerable state-level variation. The reported increase in prenatal substance exposure in the majority of US states (38) suggest that substances other than opioids are influencing this trend. Medicaid-led initiatives can be used to identify women with substance use and connect them to services.
Keywords: Neonatal abstinence syndrome; Prenatal; Substance use.
Plain language summary
What is already known about the topic? Neonatal Abstinence Syndrome (NAS) and prenatal substance exposure are significant risk factors for poor neurodevelopmental and mental health outcomes in early childhood. NAS birth rates have been increasing in the US since 2000 and the majority of NAS births are covered by Medicaid.What this article adds? This article estimates national and state-level prenatal substance exposure and NAS rates among Medicaid-covered infants born between 2016-2020 using data from the Transformed Medicaid Statistical Information System. This is the first study using post-2017 data to estimate national NAS rates. The findings can inform future federal and state policy efforts to improve access to screening, diagnosis and treatment among pregnant women with substance use disorder and infants with NAS.
© 2023. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures
References
-
- Ali M.M., Nye E., and West K., (2020). Trends in Hospital Readmission and Emergency Department Visit among Infants Born with Neonatal Abstinence Syndrome, U.S. Department of Health and Human Services, https://aspe.hhs.gov/reports/trends-hospital-readmission-emergency-depar.... Accessed 26 September 2022.
-
- Batra K, Cruz P, Cross C, Bhandari N, Abdulla F, Pharr J, et al. Incidence of neonatal abstinence syndrome epidemic and associated predictors in Nevada: A statewide audit, 2016–2018. International Journal of Environmental Research and Public Health. 2021;18(1):232. doi: 10.3390/ijerph18010232. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
