

Impact of bone and cartilage segmentation from CT and MRI on both bone forearm osteotomy planning
- PMID: 37219804
- PMCID: PMC10632286
- DOI: 10.1007/s11548-023-02929-8
Impact of bone and cartilage segmentation from CT and MRI on both bone forearm osteotomy planning
Abstract
Introduction: The use of MRI scans for pre-operative surgical planning of forearm osteotomies provides additional information of joint cartilage and soft tissue structures and reduces radiation exposure in comparison with the use of CT scans. In this study, we investigated whether using 3D information obtained from MRI with and without cartilage information leads to a different outcome of pre-operative planning.
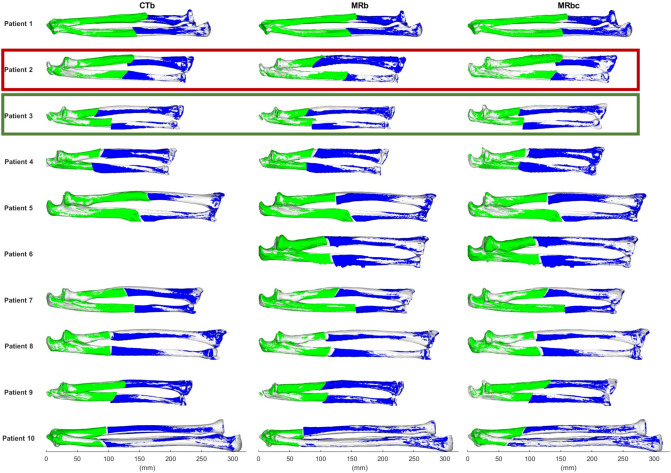
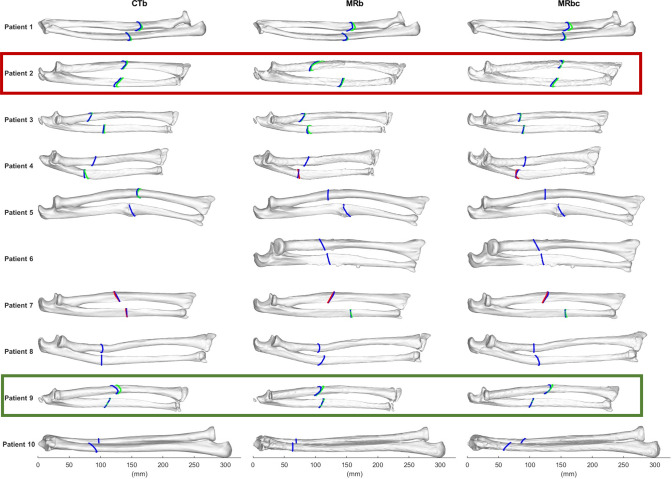
Methods: Bilateral CT and MRI scans of the forearms of 10 adolescent and young adult patients with a unilateral bone deformation were acquired in a prospective study. The bones were segmented from CT and MRI, and cartilage only from MRI. The deformed bones were virtually reconstructed, by registering the joint ends to the healthy contralateral side. An optimal osteotomy plane was determined that minimized the distance between the resulting fragments. This process was performed in threefold: using the CT and MRI bone segmentations, and the MRI cartilage segmentations.
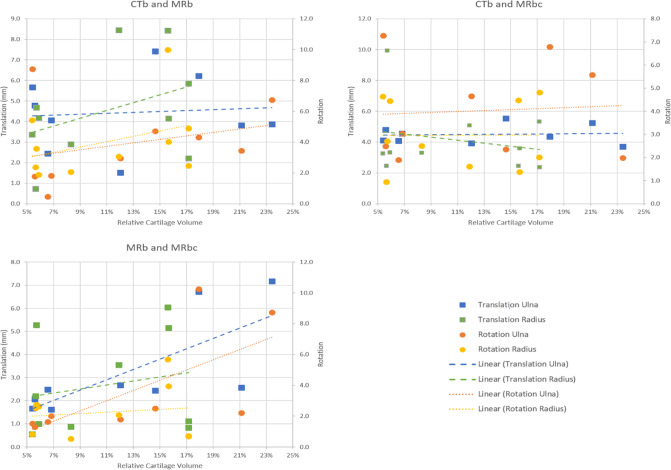
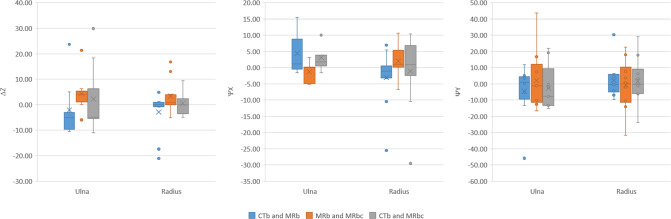
Results: Comparison of bone segmentation from MRI and CT scan resulted in a 0.95 ± 0.02 Dice Similarity Coefficient and 0.42 ± 0.07 mm Mean Absolute Surface Distance. All realignment parameters showed excellent reliability across the different segmentations. However, the mean differences in translational realignment between CT and MRI bone segmentations (4.5 ± 2.1 mm) and between MRI bone and MRI bone and cartilage segmentations (2.8 ± 2.1 mm) were shown to be clinically and statistically significant. A significant positive correlation was found between the translational realignment and the relative amount of cartilage.
Conclusion: This study indicates that although bone realignment remained largely similar when using MRI with and without cartilage information compared to using CT, the small differences in segmentation could induce statistically and clinically significant differences in the osteotomy planning. We also showed that endochondral cartilage might be a non-negligible factor when planning osteotomies for young patients.
Keywords: Bone; CT; MRI; Orthopaedic planning; Osteotomy.
© 2023. The Author(s).
Conflict of interest statement
This work was partially funded by the Netherlands Organization for Scientific Research (NWO) and is part of the Applied and Engineering Sciences research program, Project Number 15479. Peter Seevinck is minority shareholder and CSO at MRIguidance B.V. Harrie Weinans is minority shareholder at UPlanner B.V. Ralph Sakkers is minority shareholder at UPlanner B.V. and independent reviewer at MRIGuidance B.V. Max Viergever is Board Member, MICCAI Society. The other authors have no relevant interests to disclose.
Figures




References
-
- de Muinck Keizer RJO, Lechner KM, Mulders MAM, Schep NWL, Eygendaal D, Goslings JC. Three-dimensional virtual planning of corrective osteotomies of distal radius malunions: a systematic review and meta-analysis. Strateg Trauma Limb Reconstr. 2017;12:77–89. doi: 10.1007/s11751-017-0284-8. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
