

Development and Validation of a Multi-institutional Nomogram of Outcomes for PSMA-PET-Based Salvage Radiotherapy for Recurrent Prostate Cancer
- PMID: 37219907
- PMCID: PMC10208140
- DOI: 10.1001/jamanetworkopen.2023.14748
Development and Validation of a Multi-institutional Nomogram of Outcomes for PSMA-PET-Based Salvage Radiotherapy for Recurrent Prostate Cancer
Abstract
Importance: Prostate-specific antigen membrane positron-emission tomography (PSMA-PET) is increasingly used to guide salvage radiotherapy (sRT) after radical prostatectomy for patients with recurrent or persistent prostate cancer.
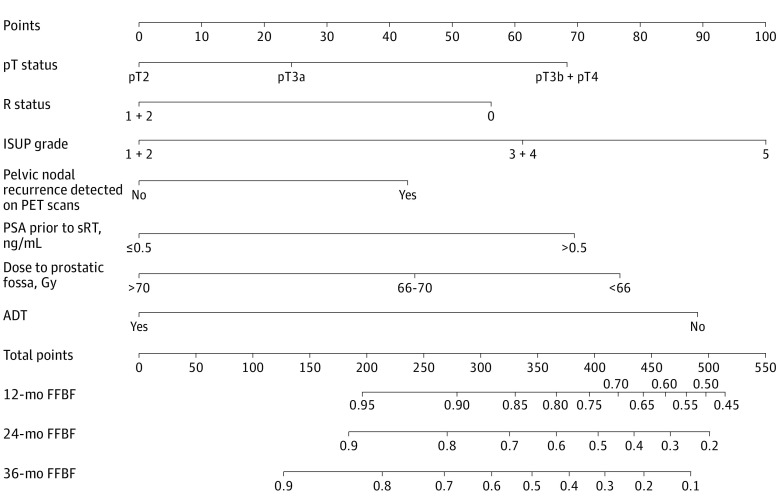
Objective: To develop and validate a nomogram for prediction of freedom from biochemical failure (FFBF) after PSMA-PET-based sRT.
Design, setting, and participants: This retrospective cohort study included 1029 patients with prostate cancer treated between July 1, 2013, and June 30, 2020, at 11 centers from 5 countries. The initial database consisted of 1221 patients. All patients had a PSMA-PET scan prior to sRT. Data were analyzed in November 2022.
Exposures: Patients with a detectable post-radical prostatectomy prostate-specific antigen (PSA) level treated with sRT to the prostatic fossa with or without additional sRT to pelvic lymphatics or concurrent androgen deprivation therapy (ADT) were eligible.
Main outcomes and measures: The FFBF rate was estimated, and a predictive nomogram was generated and validated. Biochemical relapse was defined as a PSA nadir of 0.2 ng/mL after sRT.
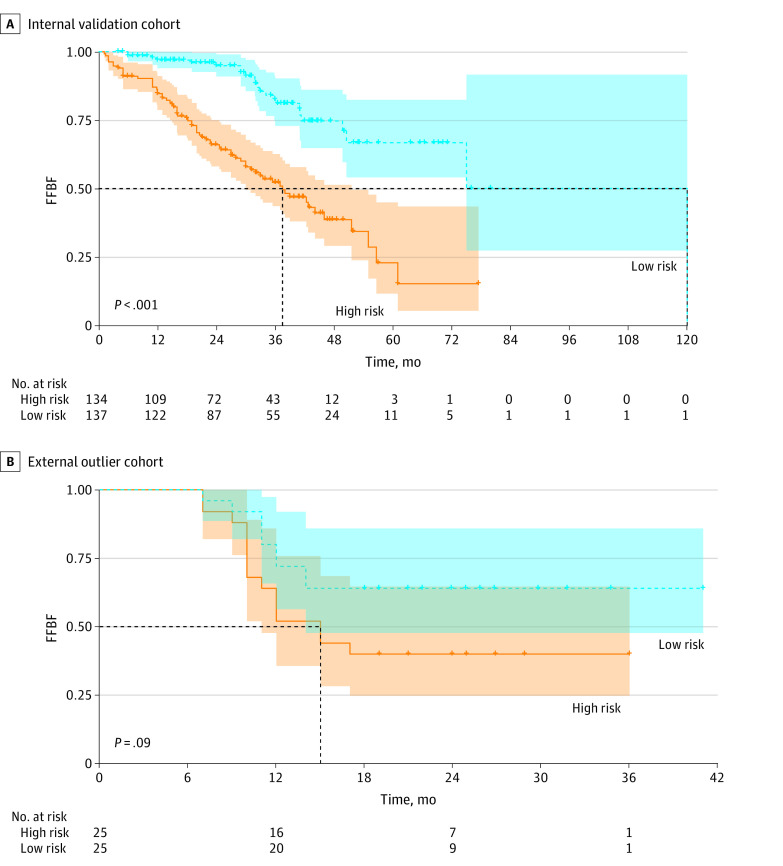
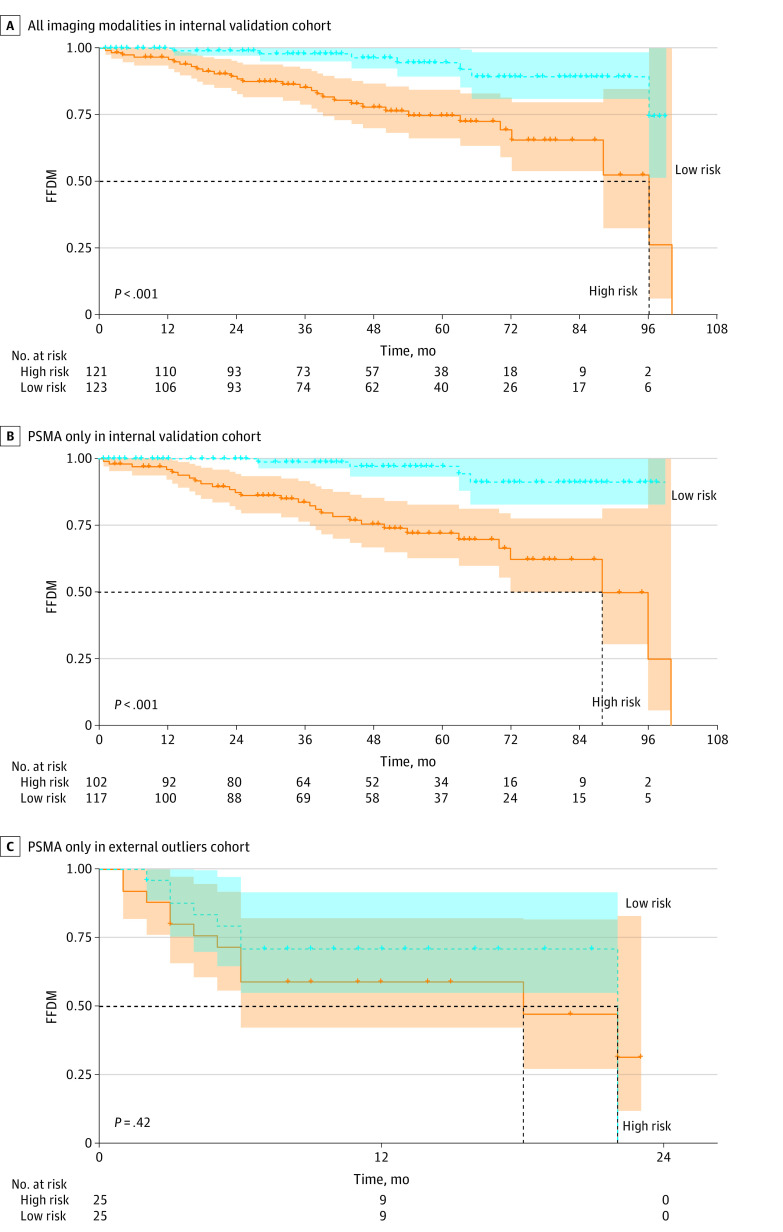
Results: In the nomogram creation and validation process, 1029 patients (median age at sRT, 70 years [IQR, 64-74 years]) were included and further divided into a training set (n = 708), internal validation set (n = 271), and external outlier validation set (n = 50). The median follow-up was 32 months (IQR, 21-45 months). Based on the PSMA-PET scan prior to sRT, 437 patients (42.5%) had local recurrences and 313 patients (30.4%) had nodal recurrences. Pelvic lymphatics were electively irradiated for 395 patients (38.4%). All patients received sRT to the prostatic fossa: 103 (10.0%) received a dose of less than 66 Gy, 551 (53.5%) received a dose of 66 to 70 Gy, and 375 (36.5%) received a dose of more than 70 Gy. Androgen deprivation therapy was given to 325 (31.6%) patients. On multivariable Cox proportional hazards regression analysis, pre-sRT PSA level (hazard ratio [HR], 1.80 [95% CI, 1.41-2.31]), International Society of Urological Pathology grade in surgery specimen (grade 5 vs 1+2: HR, 2.39 [95% CI, 1.63-3.50], pT stage (pT3b+pT4 vs pT2: HR, 1.91 [95% CI, 1.39-2.67]), surgical margins (R0 vs R1+R2+Rx: HR, 0.60 [95% CI, 0.48-0.78]), ADT use (HR, 0.49 [95% CI, 0.37-0.65]), sRT dose (>70 vs ≤66 Gy: HR, 0.44 [95% CI, 0.29-0.67]), and nodal recurrence detected on PSMA-PET scans (HR, 1.42 [95% CI, 1.09-1.85]) were associated with FFBF. The mean (SD) nomogram concordance index for FFBF was 0.72 (0.06) for the internal validation cohort and 0.67 (0.11) in the external outlier validation cohort.
Conclusions and relevance: This cohort study of patients with prostate cancer presents an internally and externally validated nomogram that estimated individual patient outcomes after PSMA-PET-guided sRT.
Conflict of interest statement
Figures

Similar articles
-
A Machine Learning Approach for Predicting Biochemical Outcome After PSMA-PET-Guided Salvage Radiotherapy in Recurrent Prostate Cancer After Radical Prostatectomy: Retrospective Study.JMIR Cancer. 2024 Sep 20;10:e60323. doi: 10.2196/60323. JMIR Cancer. 2024. PMID: 39303279 Free PMC article.
-
The prognostic significance of a negative PSMA-PET scan prior to salvage radiotherapy following radical prostatectomy.Eur J Nucl Med Mol Imaging. 2024 Jan;51(2):558-567. doi: 10.1007/s00259-023-06438-3. Epub 2023 Sep 22. Eur J Nucl Med Mol Imaging. 2024. PMID: 37736808 Free PMC article.
-
PSMA-PET/CT-guided salvage radiotherapy in recurrent or persistent prostate cancer and PSA < 0.2 ng/ml.Eur J Nucl Med Mol Imaging. 2023 Jul;50(8):2529-2536. doi: 10.1007/s00259-023-06185-5. Epub 2023 Mar 11. Eur J Nucl Med Mol Imaging. 2023. PMID: 36905411 Free PMC article.
-
Prostate-specific membrane antigen-positron emission tomography/computed tomography (PSMA-PET/CT)-guided stereotactic ablative body radiotherapy for oligometastatic prostate cancer: a single-institution experience and review of the published literature.BJU Int. 2019 Nov;124 Suppl 1:19-30. doi: 10.1111/bju.14886. Epub 2019 Sep 11. BJU Int. 2019. PMID: 31507035 Review.
-
Use of androgen deprivation and salvage radiation therapy for patients with prostate cancer and biochemical recurrence after prostatectomy.Strahlenther Onkol. 2018 Jul;194(7):619-626. doi: 10.1007/s00066-018-1269-3. Epub 2018 Jan 30. Strahlenther Onkol. 2018. PMID: 29383406 Review. English.
Cited by
-
Whole pelvis vs. hemi pelvis elective nodal radiotherapy in patients with PSMA-positive nodal recurrence after radical prostatectomy - a retrospective multi-institutional propensity score analysis.Eur J Nucl Med Mol Imaging. 2024 Oct;51(12):3770-3781. doi: 10.1007/s00259-024-06802-x. Epub 2024 Jun 28. Eur J Nucl Med Mol Imaging. 2024. PMID: 38940843 Free PMC article.
-
Impact of PSMA PET on Prostate Cancer Management.Curr Treat Options Oncol. 2024 Feb;25(2):191-205. doi: 10.1007/s11864-024-01181-9. Epub 2024 Jan 25. Curr Treat Options Oncol. 2024. PMID: 38270802 Free PMC article. Review.
-
Nomogram-based risk assessment for emergency cervical cerclage failure in patients with cervical insufficiency.Heliyon. 2024 Jun 13;10(13):e32923. doi: 10.1016/j.heliyon.2024.e32923. eCollection 2024 Jul 15. Heliyon. 2024. PMID: 39027507 Free PMC article.
-
Prostate cancer and elective nodal radiation therapy for cN0 and pN0-a never ending story? : Recommendations from the prostate cancer expert panel of the German Society of Radiation Oncology (DEGRO).Strahlenther Onkol. 2024 Mar;200(3):181-187. doi: 10.1007/s00066-023-02193-4. Epub 2024 Jan 25. Strahlenther Onkol. 2024. PMID: 38273135 Free PMC article. Review.
-
Implementation of PET/CT in radiation oncology-a patterns-of-care analysis of the German Society of Nuclear Medicine and the German Society of Radiation Oncology.Strahlenther Onkol. 2024 Nov;200(11):931-941. doi: 10.1007/s00066-024-02260-4. Epub 2024 Aug 9. Strahlenther Onkol. 2024. PMID: 39120747 Free PMC article.
References
-
- Kishan AU, Cook RR, Ciezki JP, et al. . Radical prostatectomy, external beam radiotherapy, or external beam radiotherapy with brachytherapy boost and disease progression and mortality in patients with Gleason score 9-10 prostate cancer. JAMA. 2018;319(9):896-905. doi:10.1001/jama.2018.0587 - DOI - PMC - PubMed
-
- Perera M, Papa N, Roberts M, et al. . Gallium-68 prostate-specific membrane antigen positron emission tomography in advanced prostate cancer—updated diagnostic utility, sensitivity, specificity, and distribution of prostate-specific membrane antigen–avid lesions: a systematic review and meta-analysis. Eur Urol. 2020;77(4):403-417. doi:10.1016/j.eururo.2019.01.049 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
