

Prevalence and functional profile of SARS-CoV-2 T cells in asymptomatic Kenyan adults
- PMID: 37219944
- PMCID: PMC10313370
- DOI: 10.1172/JCI170011
Prevalence and functional profile of SARS-CoV-2 T cells in asymptomatic Kenyan adults
Abstract
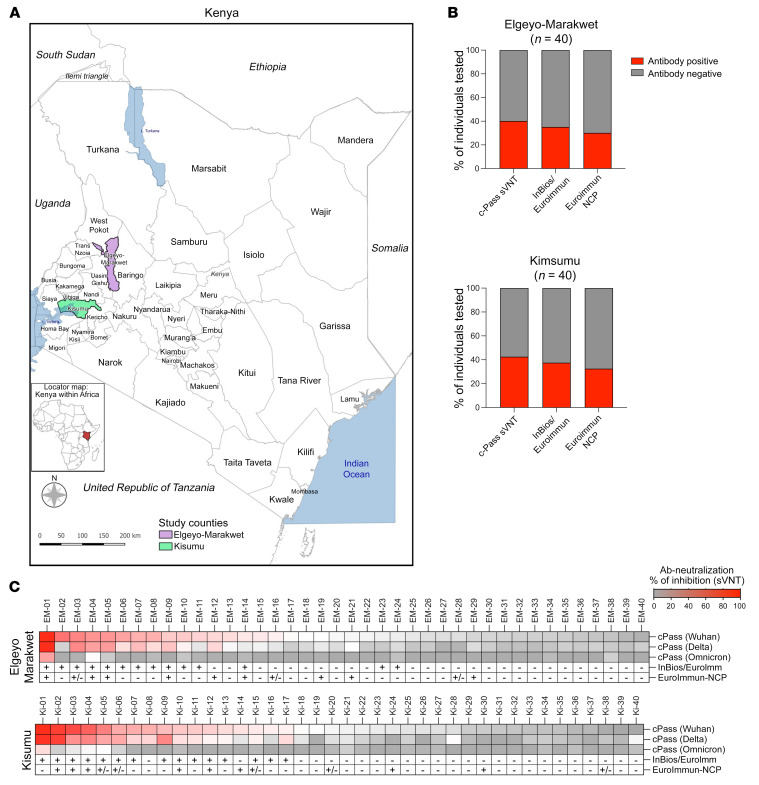
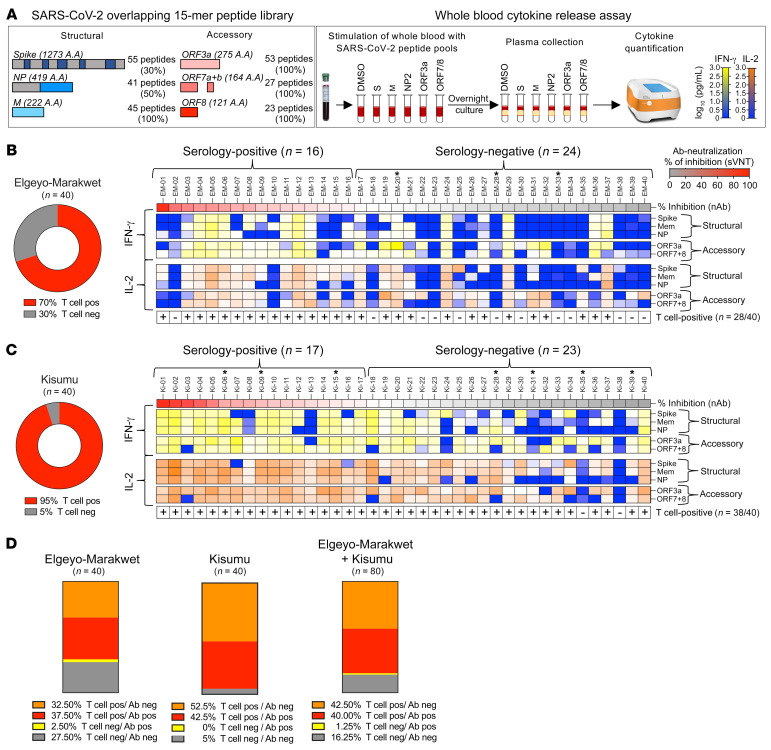
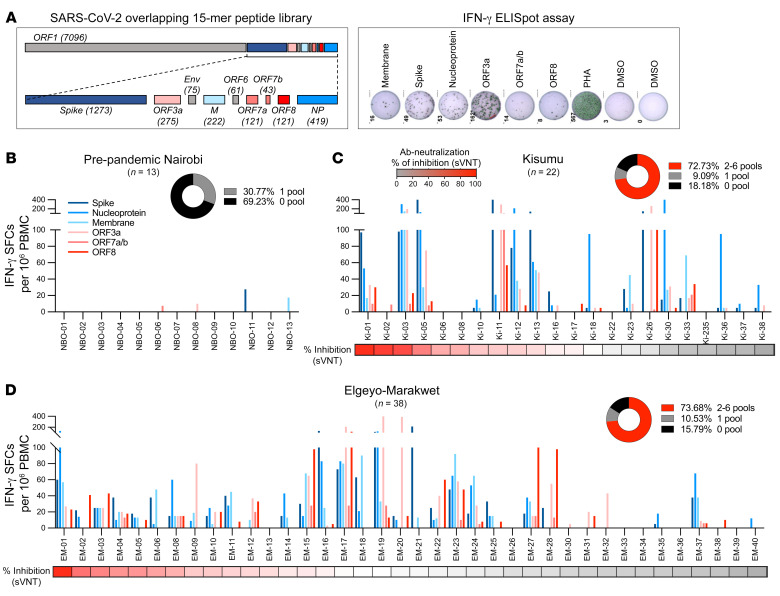
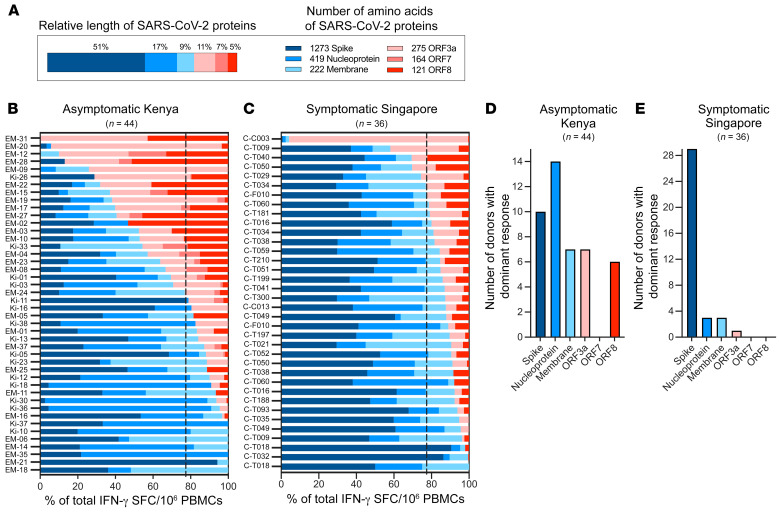
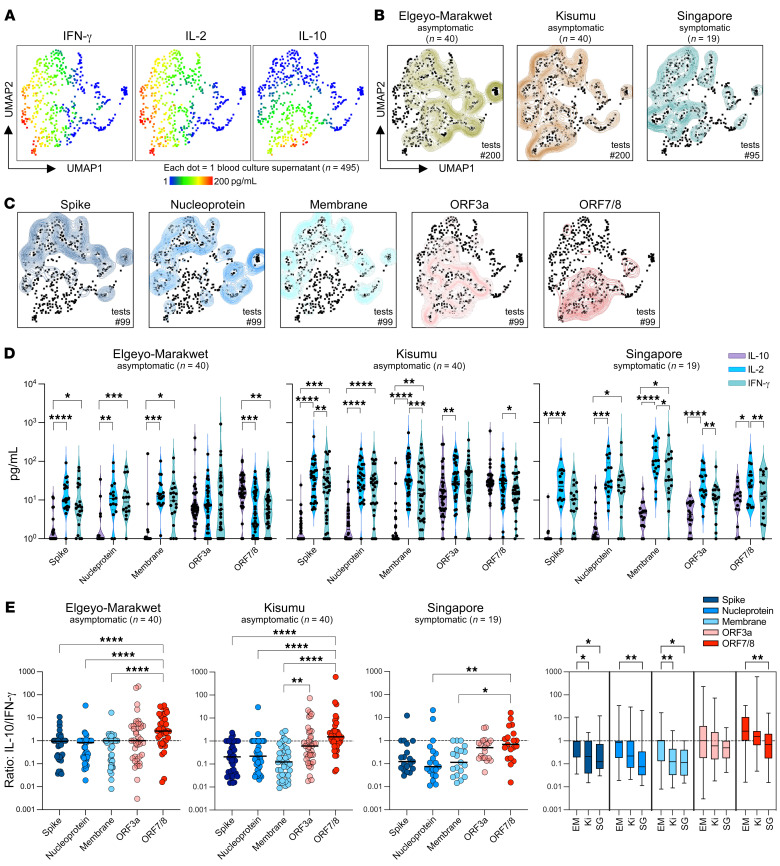
BackgroundSARS-CoV-2 infection in Africa has been characterized by a less severe disease profile than what has been observed elsewhere, but the profile of SARS-CoV-2-specific adaptive immunity in these mainly asymptomatic patients has not, to our knowledge, been analyzed.MethodsWe collected blood samples from residents of rural Kenya (n = 80), who had not experienced any respiratory symptoms or had contact with individuals with COVID-19 and had not received COVID-19 vaccines. We analyzed spike-specific antibodies and T cells specific for SARS-CoV-2 structural (membrane, nucleocapsid, and spike) and accessory (ORF3a, ORF7, ORF8) proteins. Pre-pandemic blood samples collected in Nairobi (n = 13) and blood samples from mild-to-moderately symptomatic COVID-19 convalescent patients (n = 36) living in the urban environment of Singapore were also studied.ResultsAmong asymptomatic Africans, we detected anti-spike antibodies in 41.0% of the samples and T cell responses against 2 or more SARS-CoV-2 proteins in 82.5% of samples examined. Such a pattern was absent in the pre-pandemic samples. Furthermore, distinct from cellular immunity in European and Asian COVID-19 convalescents, we observed strong T cell immunogenicity against viral accessory proteins (ORF3a, ORF8) but not structural proteins, as well as a higher IL-10/IFN-γ cytokine ratio profile.ConclusionsThe high incidence of T cell responses against different SARS-CoV-2 proteins in seronegative participants suggests that serosurveys underestimate SARS-CoV-2 prevalence in settings where asymptomatic infections prevail. The functional and antigen-specific profile of SARS-CoV-2-specific T cells in African individuals suggests that environmental factors can play a role in the development of protective antiviral immunity.FundingUS Centers for Disease Control and Prevention, Division of Global Health Protection; the Singapore Ministry of Health's National Medical Research Council (COVID19RF3-0060, COVID19RF-001, COVID19RF-008, MOH-StaR17Nov-0001).
Keywords: COVID-19; Infectious disease; T cells.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
