

On-Site Nurse-Led Cancer Genetics Program Increases Cancer Genetic Testing Completion in Black Veterans
- PMID: 37220320
- PMCID: PMC10424905
- DOI: 10.1200/OP.22.00738
On-Site Nurse-Led Cancer Genetics Program Increases Cancer Genetic Testing Completion in Black Veterans
Abstract
Purpose: Telegenetics services can expand access to guideline-recommended cancer genetic testing. However, access is often not distributed equitably to all races and ethnicities. We evaluated the impact of an on-site nurse-led cancer genetics service in a diverse Veterans Affairs Medical Center (VAMC) oncology clinic on likelihood of germline testing (GT) completion.
Methods: We conducted an observational retrospective cohort study of patients who were referred for cancer genetics services at the Philadelphia VAMC between October 1, 2020, and February 28, 2022. We evaluated the association between genetics service (on-site v telegenetics) and likelihood of GT completion in a subcohort of new consults, excluding patients with prior consults and those referred for known history of germline mutations.
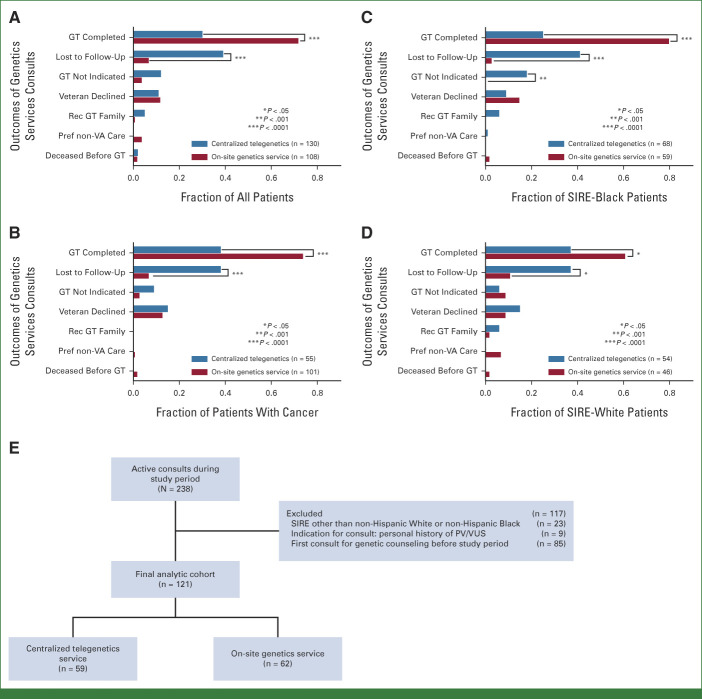
Results: A total of 238 Veterans, including 108 (45%) seen on site, were identified for cancer genetics services during the study period, with the majority referred for a personal (65%) or family (26%) history of cancer. In the subcohort of new consults, 121 Veterans (54% self-identified race/ethnicity [SIRE]-Black), including 60 (50%) seen on site, were included in the analysis of germline genetic testing completion. In a univariate analysis, patients who were seen by the on-site genetics service had 3.2-fold higher likelihood of completing GT (relative risk, 3.22; 95% CI, 1.89 to 5.48) compared with the telegenetics service. In multivariable regression analysis, the on-site genetics service was associated with higher likelihood of GT completion, but this association was only statistically significant in SIRE-Black compared with SIRE-White Veterans (adjusted RR, 4.78; 95% CI, 1.53 to 14.96; P < .001; P-interaction of race × genetics service = .016).
Conclusion: An on-site nurse-led cancer genetics service embedded in a VAMC Oncology practice was associated with higher likelihood of germline genetic testing completion than a telegenetics service among self-identified Black Veterans.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (
Figures


References
-
- Daly MB, Pal T, Berry MP, et al. Genetic/familial high-risk assessment: Breast, ovarian, and pancreatic, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Cancer Netw. 2021;19:77–102. - PubMed
-
- Weiss JM, Gupta S, Burke CA, et al. NCCN Guidelines® Insights: Genetic/familial high-risk assessment: Colorectal, version 1.2021. J Natl Compr Canc Netw. 2021;19:1122–1132. - PubMed
-
- Loeb S, Li R, Sanchez Nolasco T, et al. Barriers and facilitators of germline genetic evaluation for prostate cancer. The Prostate. 2021;81:754–764. - PubMed
-
- King EM, Smith EC. Diversification of nurse practitioner practice: Genetic cancer risk assessment. J Nurse Pract. 2020;16:447–452.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
