

Case Reports
doi: 10.1002/ccr3.7291.
eCollection 2023 May.
Implant rehabilitation of a posterior maxilla with 4-mm long implants splinted to a 10-mm long implant in a patient with osteopenia taking antiresorptive drugs: A 5-year follow-up case report
Affiliations
- PMID: 37220515
- PMCID: PMC10199821
- DOI: 10.1002/ccr3.7291
Item in Clipboard
Case Reports
Implant rehabilitation of a posterior maxilla with 4-mm long implants splinted to a 10-mm long implant in a patient with osteopenia taking antiresorptive drugs: A 5-year follow-up case report
Clin Case Rep.
.
Abstract
The report describes the rehabilitation of a maxillary arch with limited bone volume in a 67-year-old female taking antiresorptives due to osteopenia. One 10-mm and two extra-short 4-mm implants were inserted, and implant-supported splinted crowns were fabricated. The 5-year follow-up showed stable bone levels, despite poor initial stability (ISQ: 14-51).
Keywords: alveolar bone loss; dental implants; maxilla; osteopenia; short dental implants; survival rate.
© 2023 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
No conflict of interest relevant to this article is reported by the authors.
Figures
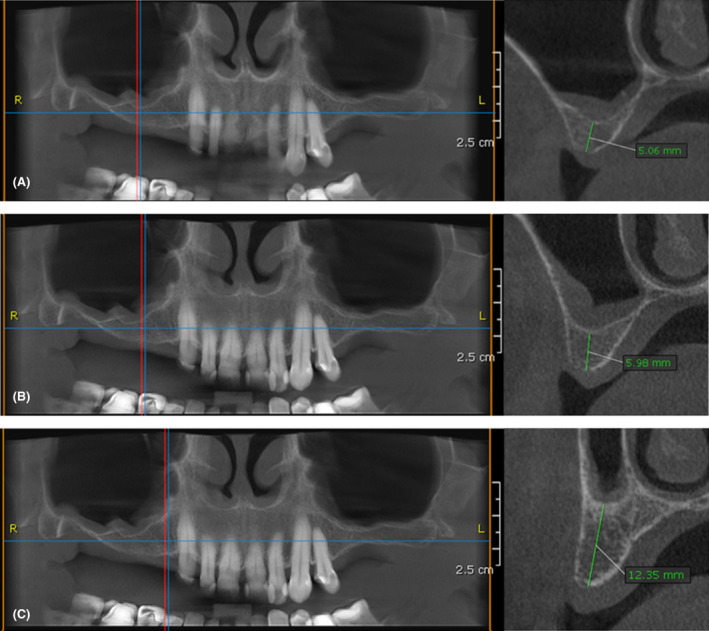
CBCT scan of the maxilla before implant placement. (A) Bone dimensions at the edentulous site of tooth no. 16. (B) Bone dimensions at the edentulous site of tooth no. 15. (C) Bone dimensions at the edentulous site of tooth no. 14.

Workflow of prosthetic rehabilitation. (A) Maxillary arch at baseline. (B) Surgical guide for dental implant placement. (C) Reflection of full‐thickness flap at the site if implant insertion. (D) Preparation of the implant beds using a surgical guide. (E) Validation of implant bed adequacy at edentulous site of former tooth no. 14. (F) Validation of implant bed adequacy at edentulous site of former tooth no. 16. (G) Insertion of implants at edentulous sites of former teeth no. 14, 15, and 16. (H) Measurement of implant stability immediately after insertion using Ostell® equipment (Integration Diagnostics). (I) Insertion of closure screws onto implants. (J) Suturing of the full‐thickness flaps. (K) Surgical site 4 days after implant insertion; secondary herpetic lesions on the palate. (L) Surgical site following suture removal, 14 days after implant insertion. (M) Surgical site 1 month after implant insertion. (N) Surgical site 6 months after implant insertion. (O) Measurement of implant stability 6 months after implant insertion using Ostell® equipment (Integration Diagnostics). (P) Positioning of open‐tray copings for the registration procedure. (Q) Implant position registration utilizing open‐tray copings and polyether impression material (Impregum®, 3 M ESPE). (R) Transfer of implant position onto a plaster cast. (S) The metal framework made of Coron®, a cobalt‐chromium alloy (Institut Straumann AG). (T) Prosthetic restoration after cementation. (U) Prosthetic restoration 1 year after cementation. (V) Prosthetic restoration 2 years after cementation. (W) Prosthetic restoration 3 years after cementation. (X) Prosthetic restoration 4 years after cementation.
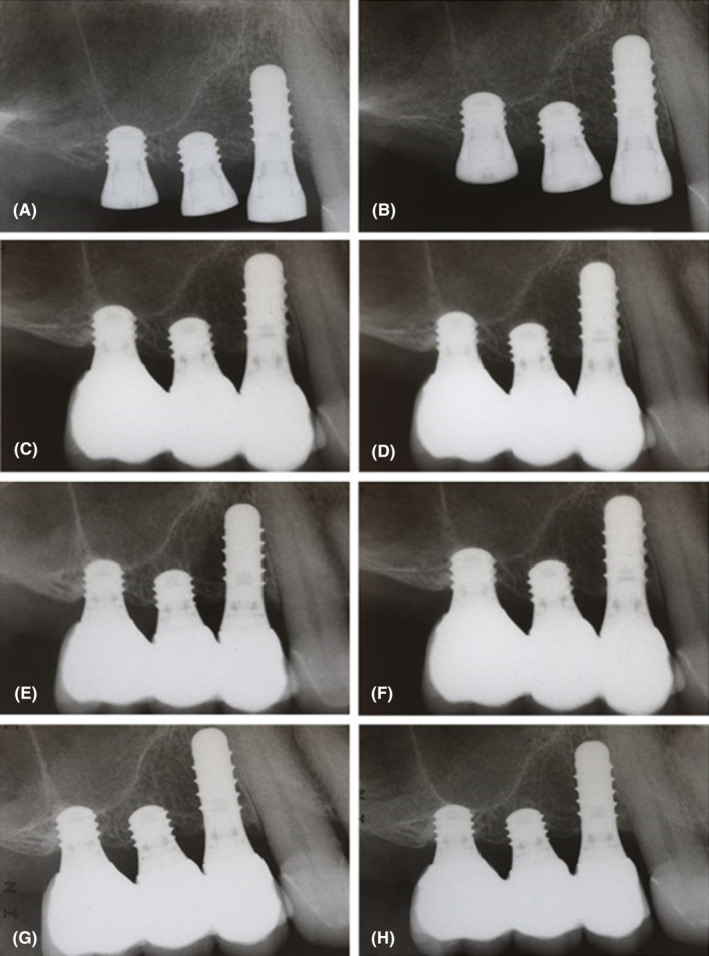
Radiographic examination of implants: (A) immediately after insertion, (B) 6 months after insertion, (C) immediately after crown cementation, (D) at the 1‐year follow‐up visit, (E) at the 2‐year follow‐up visit, (F) at the 3‐year follow‐up visit, (G) at the 4‐year follow‐up visit, (H) at the 5‐year follow‐up.

Clinical examination at the 5‐year follow‐up visit: (A) frontal view, (B) occlusion, (C) occlusal view, (D) buccal view.
References
-
- Lozano‐Carrascal N, Anglada‐Bosqued A, Salomó‐Coll O, Hernández‐Alfaro F, Wang HL, Gargallo‐Albiol J. Short implants (<8 mm) versus longer implants (≥ 8mm) with lateral sinus floor augmentation in posterior atrophic maxilla: a meta‐analysis of RCT's in humans. Med Oral Patol Oral Cir Bucal. 2020;25(2):e168‐e179. doi:10.4317/MEDORAL.23248 - DOI - PMC - PubMed
-
- Amato F, Polara G, Spedicato G. Immediate loading of fixed partial dental prostheses on extra‐short and short implants in patients with severe atrophy of the posterior maxilla or mandible: an up‐to‐4‐year clinical study. Int J Oral Maxillofac Implants. 2020;35(3):607‐615. doi:10.11607/JOMI.7943 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
