

Seasonal Malaria Chemoprevention Drug Levels and Drug Resistance Markers in Children With or Without Malaria in Burkina Faso: A Case-Control Study
- PMID: 37221018
- PMCID: PMC10547452
- DOI: 10.1093/infdis/jiad172
Seasonal Malaria Chemoprevention Drug Levels and Drug Resistance Markers in Children With or Without Malaria in Burkina Faso: A Case-Control Study
Abstract
Background: Despite scale-up of seasonal malaria chemoprevention (SMC) with sulfadoxine-pyrimethamine and amodiaquine (SP-AQ) in children 3-59 months of age in Burkina Faso, malaria incidence remains high, raising concerns regarding SMC effectiveness and selection of drug resistance. Using a case-control design, we determined associations between SMC drug levels, drug resistance markers, and presentation with malaria.
Methods: We enrolled 310 children presenting at health facilities in Bobo-Dioulasso. Cases were SMC-eligible children 6-59 months of age diagnosed with malaria. Two controls were enrolled per case: SMC-eligible children without malaria; and older (5-10 years old), SMC-ineligible children with malaria. We measured SP-AQ drug levels among SMC-eligible children and SP-AQ resistance markers among parasitemic children. Conditional logistic regression was used to compute odds ratios (ORs) comparing drug levels between cases and controls.
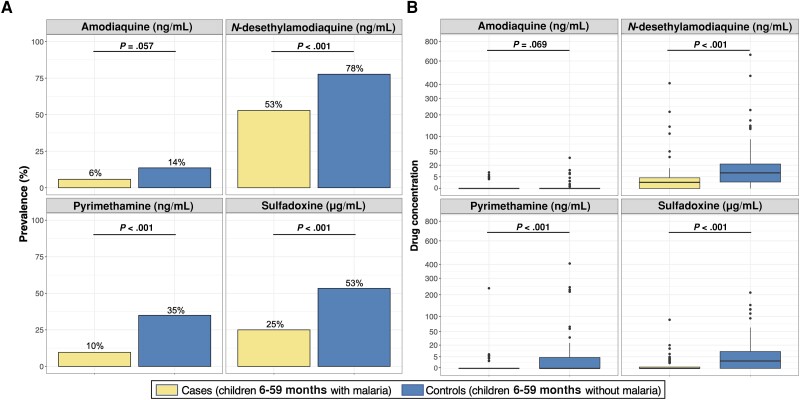
Results: Compared to SMC-eligible controls, children with malaria were less likely to have any detectable SP or AQ (OR, 0.33 [95% confidence interval, .16-.67]; P = .002) and have lower drug levels (P < .05). Prevalences of mutations mediating high-level SP resistance were rare (0%-1%) and similar between cases and SMC-ineligible controls (P > .05).
Conclusions: Incident malaria among SMC-eligible children was likely due to suboptimal levels of SP-AQ, resulting from missed cycles rather than increased antimalarial resistance to SP-AQ.
Keywords: amodiaquine; antimalarial resistance; malaria; seasonal malaria chemoprevention; sulfadoxine-pyrimethamine.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. The authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization (WHO) . WHO guidelines for malaria. Geneva, Switzerland: WHO, 2022.
-
- World Health Organization (WHO) . World malaria report 2022. Geneva, Switzerland: WHO, 2022.
