

Clinical manifestations and immune response to tuberculosis
- PMID: 37221438
- PMCID: PMC10205569
- DOI: 10.1007/s11274-023-03636-x
Clinical manifestations and immune response to tuberculosis
Abstract
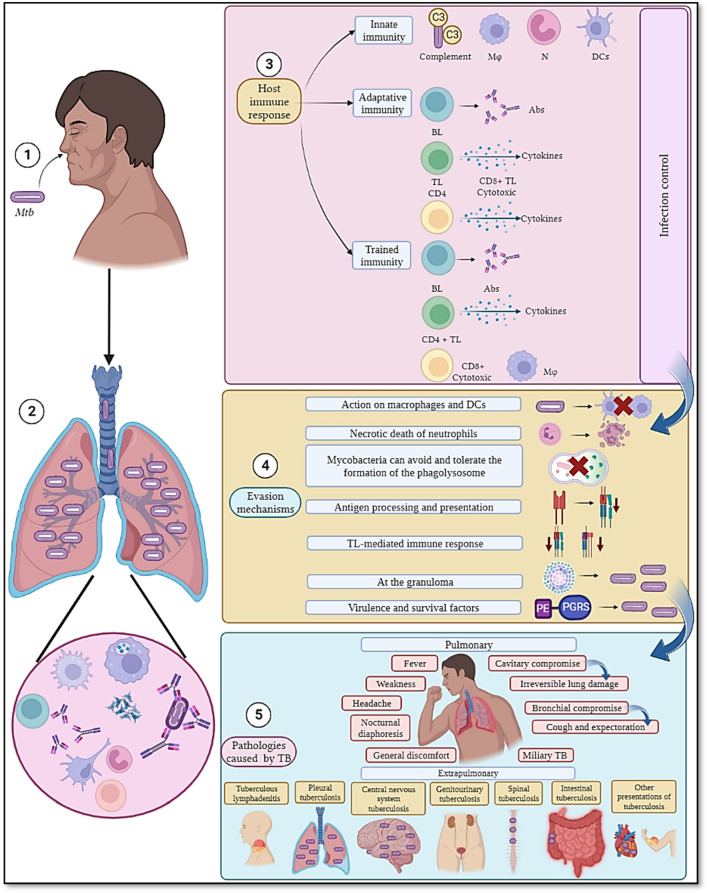
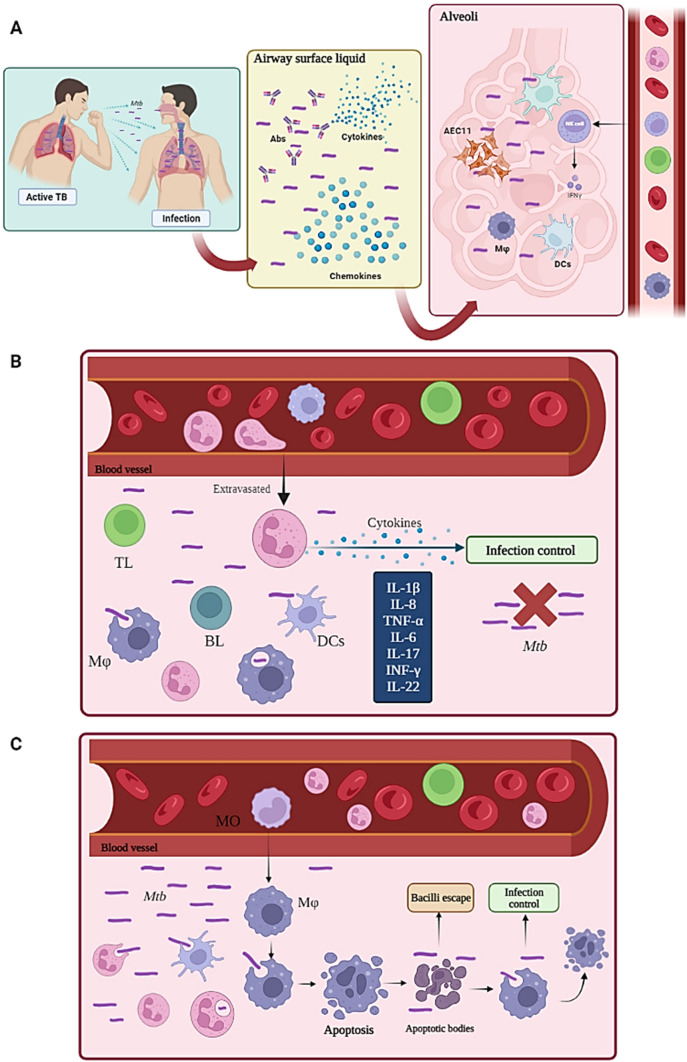
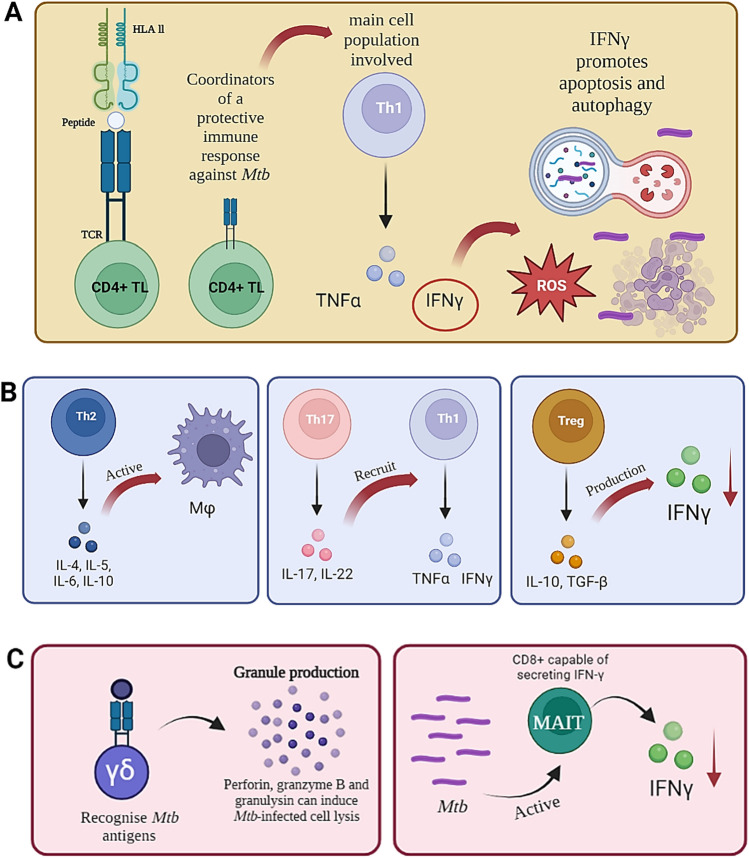
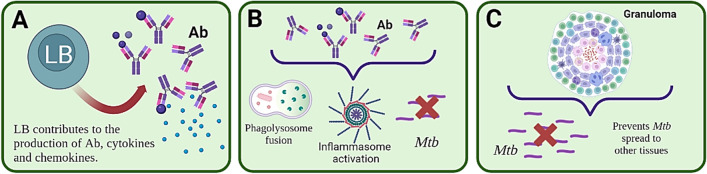
Tuberculosis is a far-reaching, high-impact disease. It is among the top ten causes of death worldwide caused by a single infectious agent; 1.6 million tuberculosis-related deaths were reported in 2021 and it has been estimated that a third of the world's population are carriers of the tuberculosis bacillus but do not develop active disease. Several authors have attributed this to hosts' differential immune response in which cellular and humoral components are involved, along with cytokines and chemokines. Ascertaining the relationship between TB development's clinical manifestations and an immune response should increase understanding of tuberculosis pathophysiological and immunological mechanisms and correlating such material with protection against Mycobacterium tuberculosis. Tuberculosis continues to be a major public health problem globally. Mortality rates have not decreased significantly; rather, they are increasing. This review has thus been aimed at deepening knowledge regarding tuberculosis by examining published material related to an immune response against Mycobacterium tuberculosis, mycobacterial evasion mechanisms regarding such response and the relationship between pulmonary and extrapulmonary clinical manifestations induced by this bacterium which are related to inflammation associated with tuberculosis dissemination through different routes.
Keywords: Clinical manifestations; Immune response; Mycobacterium tuberculosis; Tuberculosis.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Abdul-Aziz M, Tsolaki AG, Kouser L, Carroll MV, Al-Ahdal MN, Sim RB, Kishore U. Complement factor H interferes with Mycobacterium bovis BCG entry into macrophages and modulates the pro-inflammatory cytokine response. Immunobiology. 2016;221(9):944–952. doi: 10.1016/j.imbio.2016.05.011. - DOI - PubMed
-
- Aguilo N, Uranga S, Mata E, Tarancon R, Gómez AB, Marinova D, Otal I, Monzón M, Badiola J, Montenegro D, Puentes E, Rodríguez E, Vervenne RAW, Sombroek CC, Verreck FAW, Martín C. Respiratory immunization with a whole cell inactivated vaccine induces functional mucosal immunoglobulins against tuberculosis in mice and non-human primates. Front Microbiol. 2020 doi: 10.3389/fmicb.2020.01339. - DOI - PMC - PubMed
-
- Alzayer Z, Al Nasser (2022) Primary Lung Tuberculosis. In: StatPearls. StatPearls Publishing, Treasure Island (FL) - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- a/Fundación Instituto de Inmunología de Colombia (FIDIC), Carrera 50#26-20, Bogotá 111321, Colombia
- a/Fundación Instituto de Inmunología de Colombia (FIDIC), Carrera 50#26-20, Bogotá 111321, Colombia
- a/Fundación Instituto de Inmunología de Colombia (FIDIC), Carrera 50#26-20, Bogotá 111321, Colombia
- a/Fundación Instituto de Inmunología de Colombia (FIDIC), Carrera 50#26-20, Bogotá 111321, Colombia
- b/PhD Program in Biomedical and Biological Sciences, Universidad del Rosario, Carrera 24#63C-69, Bogotá 111221, Colombia
- c/Health Sciences Faculty, Universidad de Ciencias Aplicadas y Ambientales (UDCA), Calle 222#55-37, Bogotá 111166, Colombia
- d/Faculty of Medicine, Universidad Nacional de Colombia, Carrera 45#26-85, Bogotá 111321, Colombia
- e/Medicine Department, Hospital Universitario Mayor Mederi, Calle 24 # 29-45, Bogotá 111411. Colombia
- e/Medicine Department, Hospital Universitario Mayor Mederi, Calle 24 # 29-45, Bogotá 111411. Colombia
- f/Universidad Distrital Francisco José de Caldas, Carrera 3#26A-40, Bogotá 110311, Colombia
LinkOut - more resources
Full Text Sources
Medical
