

The association of spirometric small airways obstruction with respiratory symptoms, cardiometabolic diseases, and quality of life: results from the Burden of Obstructive Lung Disease (BOLD) study
- PMID: 37221593
- PMCID: PMC10207810
- DOI: 10.1186/s12931-023-02450-1
The association of spirometric small airways obstruction with respiratory symptoms, cardiometabolic diseases, and quality of life: results from the Burden of Obstructive Lung Disease (BOLD) study
Abstract
Background: Spirometric small airways obstruction (SAO) is common in the general population. Whether spirometric SAO is associated with respiratory symptoms, cardiometabolic diseases, and quality of life (QoL) is unknown.
Methods: Using data from the Burden of Obstructive Lung Disease study (N = 21,594), we defined spirometric SAO as the mean forced expiratory flow rate between 25 and 75% of the FVC (FEF25-75) less than the lower limit of normal (LLN) or the forced expiratory volume in 3 s to FVC ratio (FEV3/FVC) less than the LLN. We analysed data on respiratory symptoms, cardiometabolic diseases, and QoL collected using standardised questionnaires. We assessed the associations with spirometric SAO using multivariable regression models, and pooled site estimates using random effects meta-analysis. We conducted identical analyses for isolated spirometric SAO (i.e. with FEV1/FVC ≥ LLN).
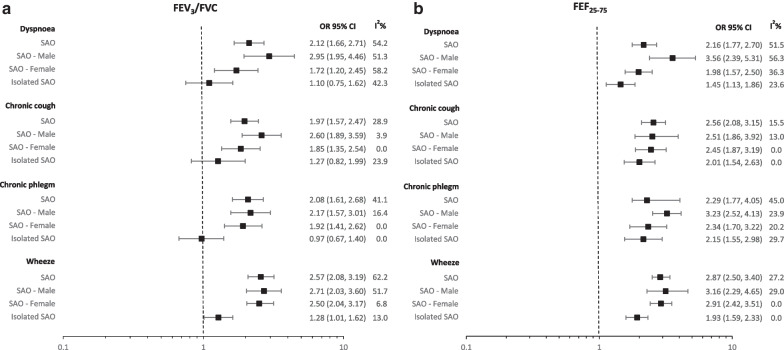
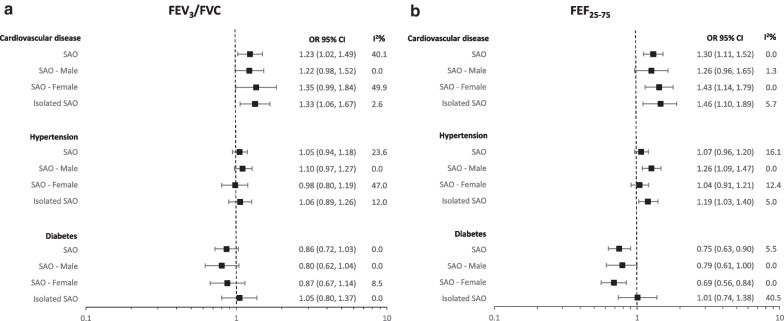
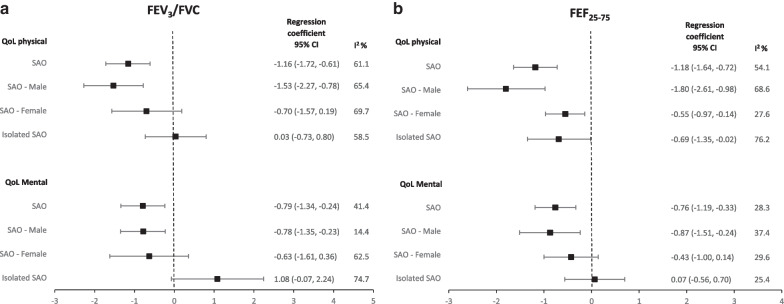
Results: Almost a fifth of the participants had spirometric SAO (19% for FEF25-75; 17% for FEV3/FVC). Using FEF25-75, spirometric SAO was associated with dyspnoea (OR = 2.16, 95% CI 1.77-2.70), chronic cough (OR = 2.56, 95% CI 2.08-3.15), chronic phlegm (OR = 2.29, 95% CI 1.77-4.05), wheeze (OR = 2.87, 95% CI 2.50-3.40) and cardiovascular disease (OR = 1.30, 95% CI 1.11-1.52), but not hypertension or diabetes. Spirometric SAO was associated with worse physical and mental QoL. These associations were similar for FEV3/FVC. Isolated spirometric SAO (10% for FEF25-75; 6% for FEV3/FVC), was also associated with respiratory symptoms and cardiovascular disease.
Conclusion: Spirometric SAO is associated with respiratory symptoms, cardiovascular disease, and QoL. Consideration should be given to the measurement of FEF25-75 and FEV3/FVC, in addition to traditional spirometry parameters.
Keywords: Cardiovascular disease; Quality of life; Small airways obstruction; Spirometry; Symptoms.
© 2023. The Author(s).
Conflict of interest statement
Outside of the submitted work: DM declares being a consultant to GlaxoSmithKline, AstraZeneca, COPD Foundation. Royalties—Up to Date. Expert Witness-Schlesinger Law Firm. All other authors declare no competing interests.
Figures
Similar articles
-
Small airways obstruction and its risk factors in the Burden of Obstructive Lung Disease (BOLD) study: a multinational cross-sectional study.Lancet Glob Health. 2023 Jan;11(1):e69-e82. doi: 10.1016/S2214-109X(22)00456-9. Lancet Glob Health. 2023. PMID: 36521955
-
A Simple Measure to Assess Hyperinflation and Air Trapping: 1-Forced Expiratory Volume in Three Second / Forced Vital Capacity.Balkan Med J. 2017 Apr 5;34(2):113-118. doi: 10.4274/balkanmedj.2015.0857. Balkan Med J. 2017. PMID: 28418337 Free PMC article.
-
Isolated small airways obstruction predicts future chronic airflow obstruction: a multinational longitudinal study.BMJ Open Respir Res. 2023 Nov;10(1):e002056. doi: 10.1136/bmjresp-2023-002056. BMJ Open Respir Res. 2023. PMID: 37989490 Free PMC article.
-
A Novel Spirometric Measure Identifies Mild COPD Unidentified by Standard Criteria.Chest. 2016 Nov;150(5):1080-1090. doi: 10.1016/j.chest.2016.06.047. Epub 2016 Jul 22. Chest. 2016. PMID: 27452770 Free PMC article.
-
Risk Factors, Morbidity, and Mortality in Association With Preserved Ratio Impaired Spirometry and Restrictive Spirometric Pattern: Clinical Relevance of Preserved Ratio Impaired Spirometry and Restrictive Spirometric Pattern.Chest. 2025 Feb;167(2):548-560. doi: 10.1016/j.chest.2024.08.026. Epub 2024 Aug 27. Chest. 2025. PMID: 39209063
Cited by
-
Small Airways Obstruction and Mortality: Findings From the UK Biobank.Chest. 2024 Oct;166(4):712-720. doi: 10.1016/j.chest.2024.04.016. Epub 2024 May 24. Chest. 2024. PMID: 38797279 Free PMC article.
-
Investigation of inert gas washout methods in a new numerical model based on an electrical analogy.Med Biol Eng Comput. 2025 Feb;63(2):447-466. doi: 10.1007/s11517-024-03200-1. Epub 2024 Oct 7. Med Biol Eng Comput. 2025. PMID: 39373835 Free PMC article.
-
Mortality risk associated with occupational exposures in people with small airways obstruction.PLoS One. 2024 Jun 11;19(6):e0305125. doi: 10.1371/journal.pone.0305125. eCollection 2024. PLoS One. 2024. PMID: 38861560 Free PMC article.
-
Long COVID symptoms after 8-month recovery: persistent static lung hyperinflation associated with small airway dysfunction.Respir Res. 2024 May 15;25(1):209. doi: 10.1186/s12931-024-02830-1. Respir Res. 2024. PMID: 38750527 Free PMC article.
-
Small airway dysfunction links asthma exacerbations with asthma control and health-related quality of life.Respir Res. 2024 Aug 12;25(1):306. doi: 10.1186/s12931-024-02937-5. Respir Res. 2024. PMID: 39135076 Free PMC article.
References
-
- Weibel ER. Morphometry of the human lung. Saint Louis: Elsevier Science & Technology; 1963.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
