

Feasibility of telerehabilitation for heart failure patients inaccessible for outpatient rehabilitation
- PMID: 37221704
- PMCID: PMC10375147
- DOI: 10.1002/ehf2.14405
Feasibility of telerehabilitation for heart failure patients inaccessible for outpatient rehabilitation
Abstract
Aims: Despite strong recommendations, outpatient cardiac rehabilitation is underused in chronic heart failure (CHF) patients. Possible barriers are frailty, accessibility, and rural living, which may be overcome by telerehabilitation. We designed a randomized, controlled trial to evaluate the feasibility of a 3-month real-time, home-based telerehabilitation, high-intensity exercise programme for CHF patients who are either unable or unwilling to participate in standard outpatient cardiac rehabilitation and to explore outcomes of self-efficacy and physical fitness at 3 months post-intervention.
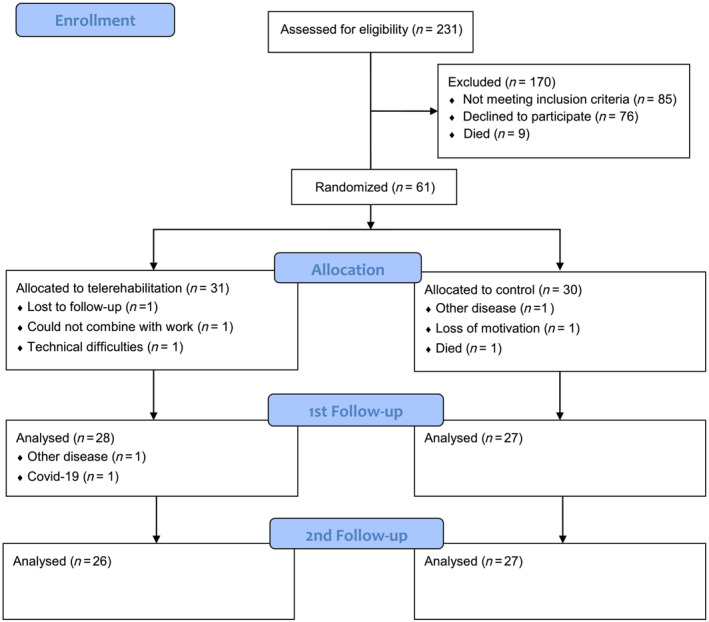
Methods and results: CHF patients with reduced (≤40%), mildly reduced (41-49%), or preserved ejection fraction (≥50%) (n = 61) were randomized 1:1 to telerehabilitation or control in a prospective controlled trial. The telerehabilitation group (n = 31) received real-time, home-based, high-intensity exercise for 3 months. Inclusion criteria were (i) ≥18 years, (ii) New York Heart Association class II-III, stable on optimized medical therapy for >4 weeks, and (iii) N-terminal pro-brain natriuretic peptide >300 ng/L. All participants participated in a 2-day 'Living with heart failure' course. No other intervention beyond standard care was provided for controls. Outcome measures were adherence, adverse events, self-reported outcome measures, the general perceived self-efficacy scale, peak oxygen uptake (VO2peak ) and a 6-min walk test (6MWT). The mean age was 67.6 (11.3) years, and 18% were women. Most of the telerehabilitation group (80%) was adherent or partly adherent. No adverse events were reported during supervised exercise. Ninety-six per cent (26/27) reported that they felt safe during real-time, home-based telerehabilitation, high-intensity exercise, and 96% (24/25) reported that, after the home-based supervised telerehabilitation, they were motivated to participate in further exercise training. More than half the population (15/26) reported minor technical issues with the videoconferencing software. 6MWT distance increased significantly in the telerehabilitation group (19 m, P = 0.02), whereas a significant decrease in VO2peak (-0.72 mL/kg/min, P = 0.03) was observed in the control group. There were no significant differences between the groups in general perceived self-efficacy scale, VO2peak , and 6MWT distance after intervention or at 3 months post-intervention.
Conclusions: Home-based telerehabilitation was feasible in chronic heart failure patients inaccessible for outpatient cardiac rehabilitation. Most participants were adherent when given more time and felt safe exercising at home under supervision, and no adverse events occurred. The trial suggests that telerehabilitation can increase the use of cardiac rehabilitation, but the clinical benefit of telerehabilitation must be evaluated in larger trials.
Trial registration: ClinicalTrials.gov NCT03183323.
Keywords: Cardiopulmonary exercise test; Exercise training; Heart failure; Physical activity; VO2.
© 2023 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Ponikowski P, Anker SD, AlHabib KF, Cowie MR, Force TL, Hu S, Jaarsma T, Krum H, Rastogi V, Rohde LE, Samal UC, Shimokawa H, Budi Siswanto B, Sliwa K, Filippatos G. Heart failure: preventing disease and death worldwide. ESC Heart Fail. 2014; 1: 4–25. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
