

Current trends in rehabilitation of rotator cuff injuries
- PMID: 37222530
- PMCID: PMC10208043
- DOI: 10.1051/sicotj/2023011
Current trends in rehabilitation of rotator cuff injuries
Abstract
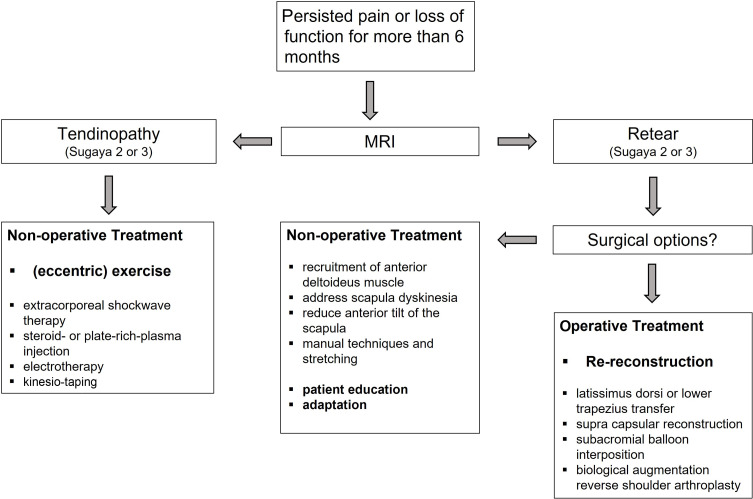
Rehabilitation has a fundamental role in the management of rotator cuff pathology whether the final choice is conservative or surgical treatment. Conservative treatment can give excellent results in cases of rotator cuff tendinopathies without rupture, partial tears less than 50% of the thickness of the tendon, chronic full-thickness tears in elderly patients and irreparable tears. It is an option prior to reconstructive surgery in non-pseudo paralytic cases. When surgery is indicated, adequate postoperative rehabilitation is the best complement to obtain a successful result. No consensus has still been established on the optimal postoperative protocol to follow. No differences were found between delayed, early passive and early active protocols after rotator cuff repair. However, early motion improved the range of motion in the short and mid-term, allowing faster recovery. A 5-phase postoperative rehabilitation protocol is described. Rehabilitation is also an option in specific failed surgical procedures. To choose a therapeutic strategy in these cases, it is reasonable to differentiate between Sugaya type 2 or 3 (tendinopathy of the tendon) and type 4 or 5 (discontinuity/retear). The rehabilitation program should always be tailored to the individual patient.
Keywords: Rehabilitation; Rehabilitation protocol; Rotator cuff; Rotator cuff repair; Shoulder.
© The Authors, published by EDP Sciences, 2023.
Conflict of interest statement
All authors certify that they have no financial conflict of interest (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) in connection with this article.
Figures
References
-
- Codman EA (1934) Calcified deposits in the Supraspinatus tendon. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or about the Subacromial Bursa. Boston, Thomas Todd Co.
-
- Matsen FA, Titelman RM, Lippit SB, Wirth MA, Rockwood CA (2004) Rotator cuff In: The Shoulder, 3rd edn. Rockwood CA Jr, Matsen FA III, Wirth MA, Lippitt SB, Editors. Philadelphia, PA, Saunders.
-
- Rockwood CA, Lyons FR (1993) Shoulder impingement syndrome: diagnosis, radiographic evaluation, and treatment with a modified Neer acromioplasty. J Bone Joint Surg Am 75(3), 409–424. - PubMed
-
- Burkhead WZ, Rockwood CA (1992) Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am, 74, 890–896. - PubMed
-
- Lewis JS, Cook CE, Hoffmann TC, O’Sullivan P (2020) The elephant in the room: too much medicine in musculoskeletal practice. J Orthop Sports Phys Ther 50(1), 1–4. - PubMed
LinkOut - more resources
Full Text Sources