

Towards Novel HIV-1 Serodiagnostic Tests without Vaccine-Induced Seroreactivity
- PMID: 37222611
- PMCID: PMC10269835
- DOI: 10.1128/spectrum.00715-23
Towards Novel HIV-1 Serodiagnostic Tests without Vaccine-Induced Seroreactivity
Abstract
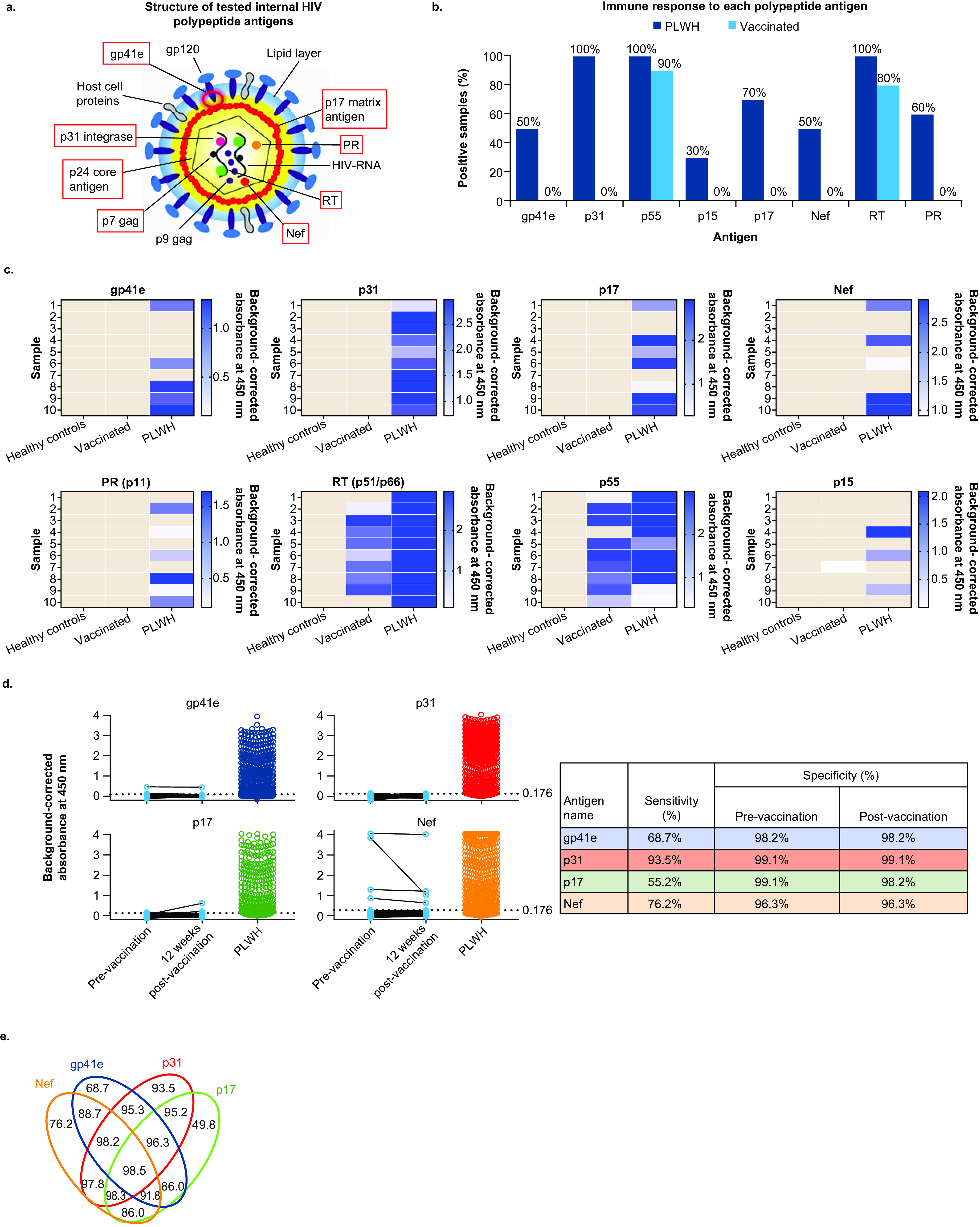
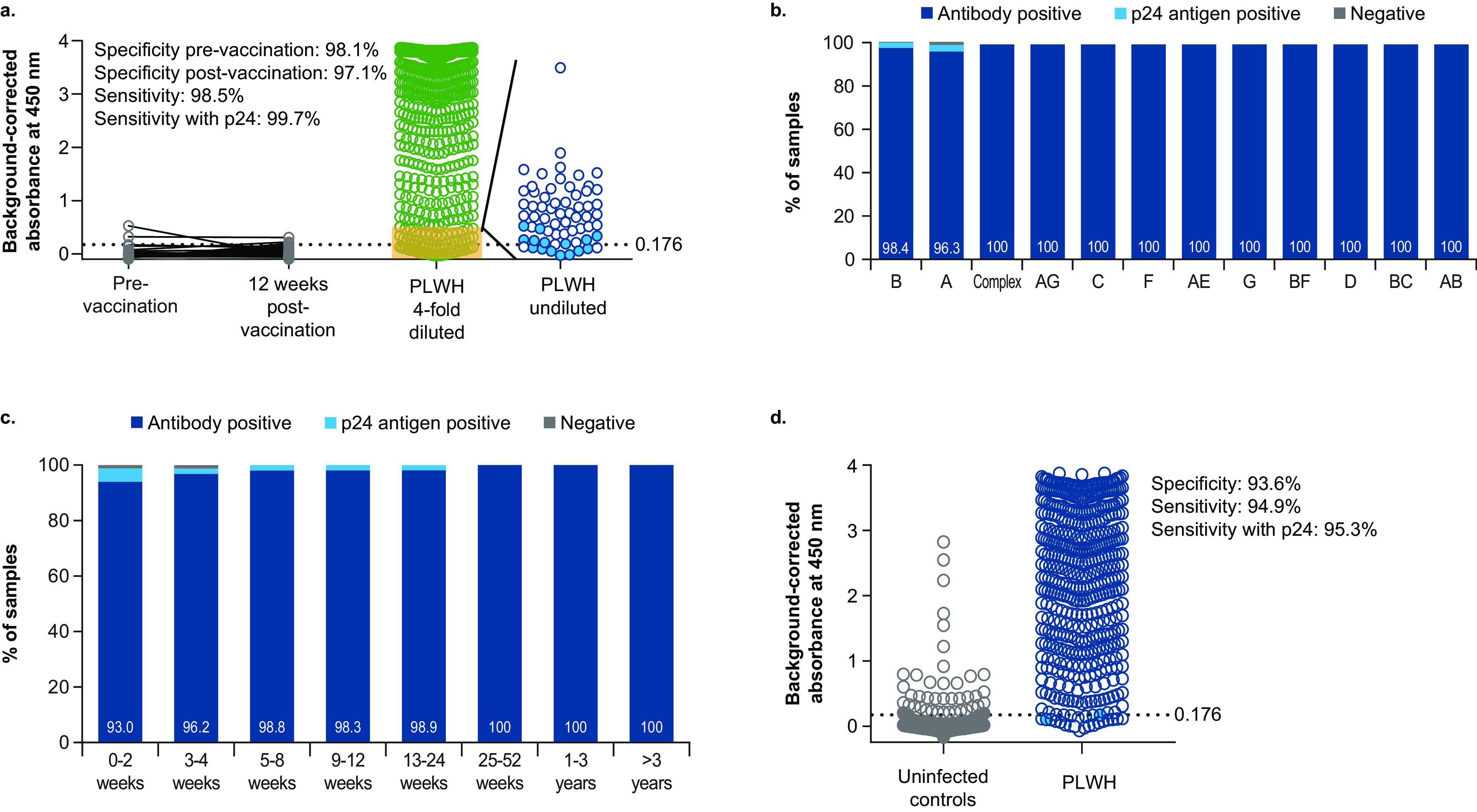
Vaccine-induced seroreactivity/positivity (VISR/P) poses a significant and common challenge to HIV vaccine implementation, as up to 95% of vaccine recipients may be misclassified as having HIV infection by current HIV screening and confirmatory serological assays. We investigated whether internal HIV proteins could be used to overcome VISR and discovered a set of 4 antigens (gp41 endodomain, p31 integrase, p17 matrix protein, and Nef) that are recognized by antibodies produced in individuals with HIV infection but not in vaccinated individuals. When evaluated in a multiplex double-antigen bridging ELISA, this antigen combination had specificities of 98.1% prevaccination and 97.1% postvaccination, demonstrating the assay is minimally impacted by vaccine-induced antibodies. The sensitivity was 98.5%, further increasing to 99.7% when p24 antigen testing was included. Results were similar across HIV-1 clades. Although more technical advancements will be desired, this research provides the groundwork for the development of new fourth-generation HIV tests unaffected by VISR. IMPORTANCE While the detection of HIV infection is accomplished by several methods, the most common are serological tests that detect host antibodies produced in response to viral infection. However, the use of current serological tests may present a significant challenge to the adoption of an HIV vaccine in the future because the antibodies to HIV antigens detected in currently available tests also tend to be included as antigens in the HIV vaccines in development. The use of these serological tests may thus result in the misclassification of vaccinated HIV-negative individuals, which can have potential for significant harms for individuals and could prevent the widespread adoption and implementation of HIV vaccines. Our study aimed to identify and evaluate target antigens for inclusion in new serological tests that can be used to identify HIV infections without interference from vaccine-induced antibodies but also fit within existing platforms for HIV diagnostics.
Keywords: antigens; diagnostics; human immunodeficiency virus; seroreactivity; vaccine.
Conflict of interest statement
The authors declare a conflict of interest. O.L., J.V., and W.C. are current employees of Janssen Pharmaceutica NV, and D.J.S., V.O.M., and M.G.P. are current employees of Janssen Vaccines & Prevention B.V., both being Johnson & Johnson Companies and they may own stock or stock options in that company. L.L. is a consultant for Janssen Vaccines and Prevention B.V. The remaining co-authors have no conflicts of interest with the content of this article.
Figures


References
-
- UNAIDS. 2020. UNAIDS data 2020. https://www.unaids.org/sites/default/files/media_asset/2020_aids-data-bo....
-
- Dopel SH, Schubert U, Grunow R, Pas P, Ronspeck W, Pauli G, Porstmann T. 1991. Comparison of four anti-HIV screening assays which belong to different test generations. Eur J Clin Chem Clin Biochem 29:331–337. - PubMed
-
- Manocha M, Chitralekha KT, Thakar M, Shashikiran D, Paranjape RS, Rao DN. 2003. Comparing modified and plain peptide linked enzyme immunosorbent assay (ELISA) for detection of human immunodeficiency virus type-1 (HIV-1) and type-2 (HIV-2) antibodies. Immunol Lett 85:275–278. doi: 10.1016/s0165-2478(02)00257-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
