

Clinical Utility of Deucravacitinib for the Management of Moderate to Severe Plaque Psoriasis
- PMID: 37223005
- PMCID: PMC10202110
- DOI: 10.2147/TCRM.S388324
Clinical Utility of Deucravacitinib for the Management of Moderate to Severe Plaque Psoriasis
Abstract
Introduction: Psoriasis is a chronic, immune-mediated skin condition with significant detriments to physical/mental health. While systemic therapies are available for the treatment of moderate-to-severe psoriasis, patients can experience therapeutic failure, loss of efficacy, or medical contraindications that require other therapeutic options.
Objective: With the recent approval of deucravacitinib, a first-in-class TYK2 small molecule inhibitor administered orally for psoriasis patients, we reviewed data from randomized controlled trials (RCTs) to synthesize its clinical utility. To our knowledge, this is the first systematic review and meta-analysis of deucravacitinib comparing its clinical efficacy to placebo in psoriasis.
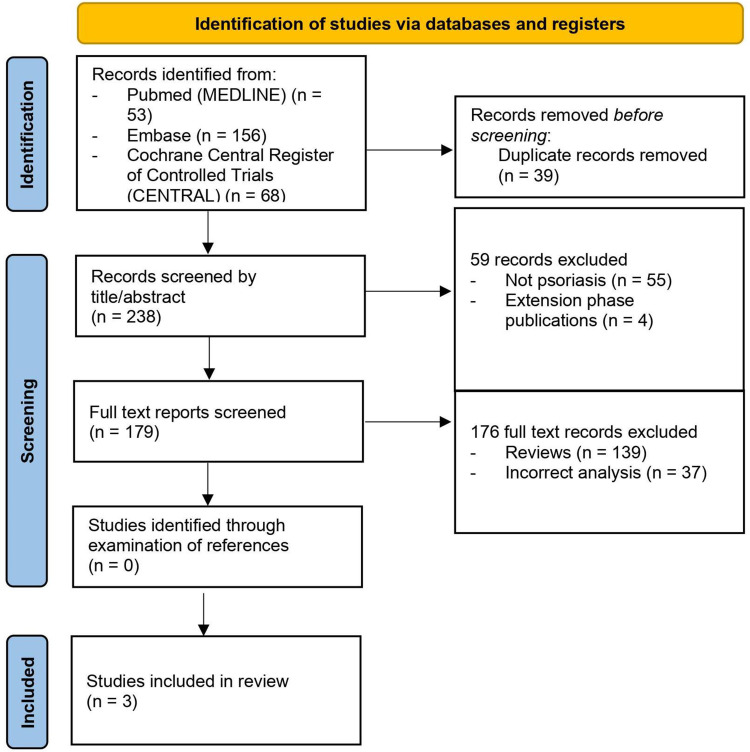
Methods: A literature search was conducted in PubMed (MEDLINE), Embase, and the Cochrane Central Register of Controlled Trials to identify RCTs studying deucravacitinib in human patients with moderate-to-severe psoriasis.
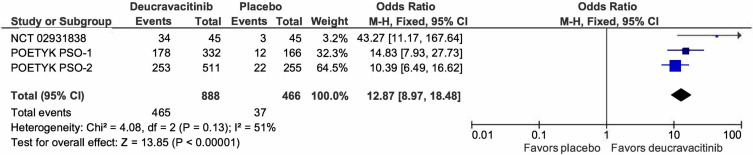
Results: One placebo-controlled Phase II RCT and two placebo-controlled/active-comparator Phase III RCTs were included for review. Patients (N=1953) treated with deucravacitinib 6 mg daily showed marked improvement in disease severity (Psoriasis Area and Severity Index (PASI), static Physician Global Assessment (sPGA) and quality-of-life outcomes compared to patients administered comparator (apremilast) and placebo. Clinical improvement given deucravacitinib was noted for scalp psoriasis but not fingernail psoriasis. Meta-analysis (deucravacitinib, n=888; placebo, n=466) comparing rates of clearance (sPGA 0/1) demonstrated superior efficacy of deucravacitinib compared to placebo (odds ratio, 12.87; 95% confidence interval, 8.97-18.48; χ2=4.08, I2=51%). Deucravacitinib was well-tolerated, with similar rate of occurrence and type of adverse events reported among patients treated with placebo or apremilast at Week 12-16. No cardiovascular events, serious infections, or lab abnormalities were noted.
Conclusion: Deucravacitinib possesses good efficacy, with no report of safety concerns associated with prior JAK inhibitors used for psoriasis. Meta-analysis demonstrated deucravacitinib's superiority compared to placebo, indicating its promising clinical utility. Further studies are needed to observe long-term safety and efficacy, and to compare deucravacitinib to existing treatments.
Keywords: apremilast; deucravacitinib; meta-analysis; placebo; plaque psoriasis; systematic review.
© 2023 Jin et al.
Conflict of interest statement
J.Q.J. has received research grant funding from the National Psoriasis Foundation and institutional funding from the University of California, San Francisco. T.B. has received research grant funding from Novartis and Regeneron and is a principal investigator for trials sponsored by Abbvie, Castle, CorEvitas, Dermavant, Galderma, Mindera, and Pfizer. T.B. has also served as an advisor for Abbvie, Arcutis, Boehringer-Ingelheim, Bristol Myers Squibb, Janssen, Leo, Lilly, Novartis, Pfizer, Sun, and UCB. W.L. has received research grant funding from Abbvie, Amgen, Janssen, Leo, Novartis, Pfizer, Regeneron, and TRex Bio. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
The efficacy and safety of tyrosine kinase 2 inhibitor deucravacitinib in the treatment of plaque psoriasis: a systematic review and meta-analysis of randomized controlled trials.Front Med (Lausanne). 2023 Sep 29;10:1264667. doi: 10.3389/fmed.2023.1264667. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37841017 Free PMC article.
-
Efficacy and safety of the selective TYK2 inhibitor, deucravacitinib, in Japanese patients with moderate to severe plaque psoriasis: Subgroup analysis of a randomized, double-blind, placebo-controlled, global phase 3 trial.J Dermatol. 2023 May;50(5):588-595. doi: 10.1111/1346-8138.16740. Epub 2023 Mar 7. J Dermatol. 2023. PMID: 36882942 Clinical Trial.
-
Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: Efficacy and safety results from the 52-week, randomized, double-blinded, placebo-controlled phase 3 POETYK PSO-1 trial.J Am Acad Dermatol. 2023 Jan;88(1):29-39. doi: 10.1016/j.jaad.2022.07.002. Epub 2022 Jul 9. J Am Acad Dermatol. 2023. PMID: 35820547 Clinical Trial.
-
Deucravacitinib versus placebo and apremilast in moderate to severe plaque psoriasis: Efficacy and safety results from the 52-week, randomized, double-blinded, phase 3 Program fOr Evaluation of TYK2 inhibitor psoriasis second trial.J Am Acad Dermatol. 2023 Jan;88(1):40-51. doi: 10.1016/j.jaad.2022.08.061. Epub 2022 Sep 14. J Am Acad Dermatol. 2023. PMID: 36115523 Clinical Trial.
-
Deucravacitinib: The First FDA-Approved Oral TYK2 Inhibitor for Moderate to Severe Plaque Psoriasis.Ann Pharmacother. 2024 Apr;58(4):416-427. doi: 10.1177/10600280231153863. Epub 2023 Jun 21. Ann Pharmacother. 2024. PMID: 37341177 Review.
Cited by
-
Biologics and Small Molecules for Inflammatory Nail Disorders: A Narrative Review.Indian Dermatol Online J. 2024 Dec 26;16(1):50-58. doi: 10.4103/idoj.idoj_445_24. eCollection 2025 Jan-Feb. Indian Dermatol Online J. 2024. PMID: 39850668 Free PMC article.
-
The treatment of psoriasis via herbal formulation and nano-polyherbal formulation: A new approach.Bioimpacts. 2024 Aug 11;15:30341. doi: 10.34172/bi.30341. eCollection 2025. Bioimpacts. 2024. PMID: 40256226 Free PMC article. Review.
-
Mechanistic Investigation of WWOX Function in NF-kB-Induced Skin Inflammation in Psoriasis.Int J Mol Sci. 2023 Dec 21;25(1):167. doi: 10.3390/ijms25010167. Int J Mol Sci. 2023. PMID: 38203337 Free PMC article.
-
Psoriasis and Molecular Target Therapies: Evidence of Efficacy in Preventing Cardiovascular Comorbidities.Dermatol Ther (Heidelb). 2024 Apr;14(4):841-852. doi: 10.1007/s13555-024-01152-w. Epub 2024 Apr 9. Dermatol Ther (Heidelb). 2024. PMID: 38592640 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
