

Clinical course of patients with adrenal incidentalomas and cortisol autonomy: a German retrospective single center cohort study
- PMID: 37223045
- PMCID: PMC10200872
- DOI: 10.3389/fendo.2023.1123132
Clinical course of patients with adrenal incidentalomas and cortisol autonomy: a German retrospective single center cohort study
Abstract
Background: Adrenal incidentalomas with cortisol autonomy are associated with increased cardiovascular morbidity and mortality. Specific data on the clinical and biochemical course of affected patients are lacking.
Methods: Retrospective study from a tertiary referral centre in Germany. After exclusion of overt hormone excess, malignancy and glucocorticoid medication, patients with adrenal incidentalomas were stratified according to serum cortisol after 1 mg dexamethasone: autonomous cortisol secretion (ACS), >5.0; possible ACS (PACS), 1.9-5.0; non-functioning adenomas (NFA), ≤1.8 µg/dl.
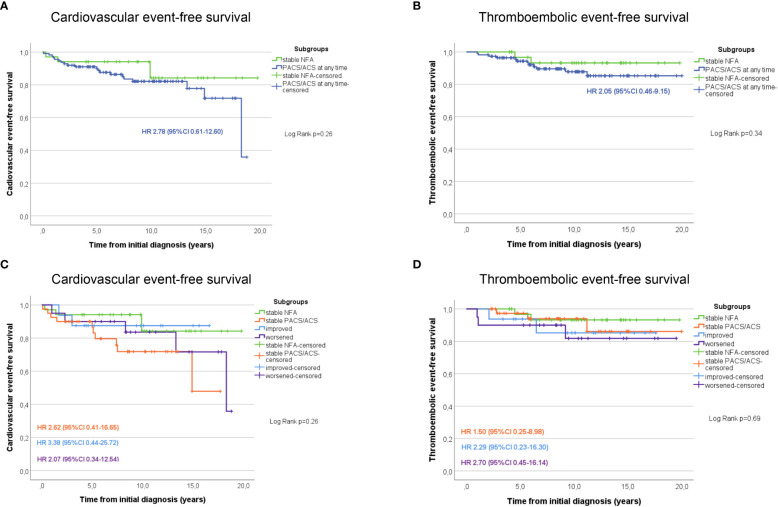
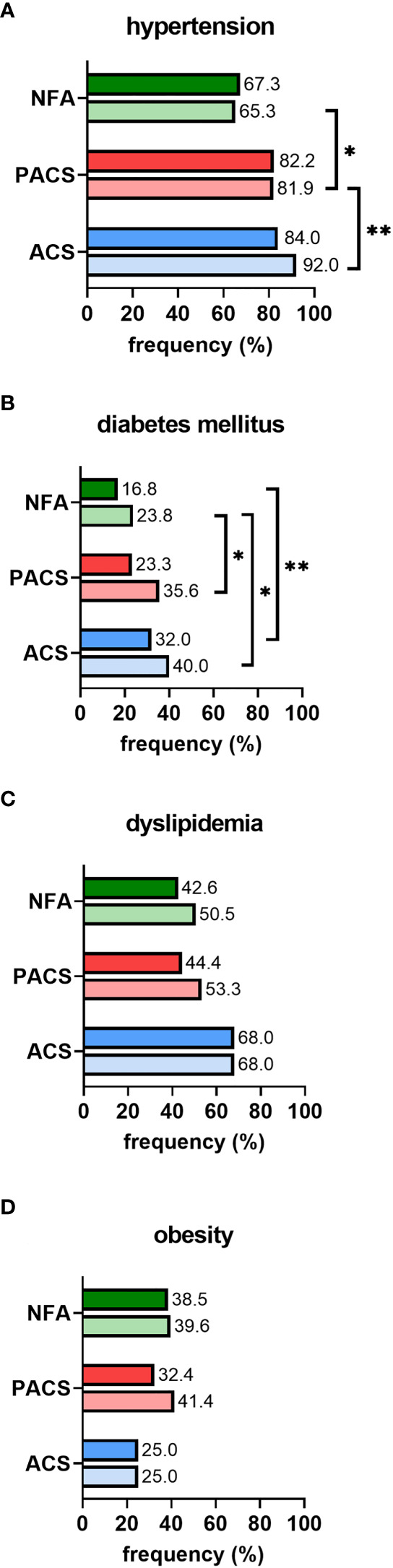
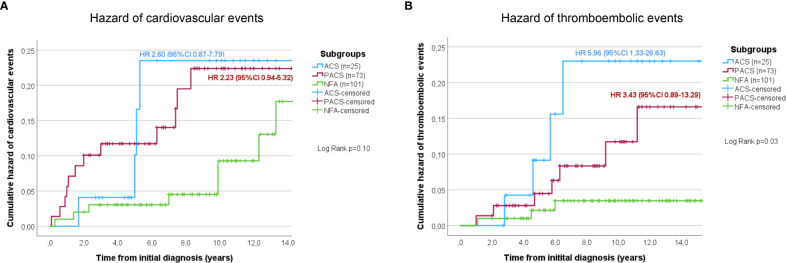
Results: A total of 260 patients were enrolled (147 women (56.5%), median follow-up 8.8 (2.0-20.8) years). At initial diagnosis, median age was 59.5 (20-82) years, and median tumour size was 27 (10-116) mm. Bilateral tumours were more prevalent in ACS (30.0%) and PACS (21.9%) than in NFA (8.1%). Over time, 40/124 (32.3%) patients had a shift of their hormonal secretion pattern (NFA to PACS/ACS, n=15/53; PACS to ACS, n=6/47; ACS to PACS, n=11/24; PACS to NFA, n=8/47). However, none of the patients developed overt Cushing's syndrome. Sixty-one patients underwent adrenalectomy (NFA, 17.9%; PACS, 24.0%; ACS, 39.0%). When non-operated patients with NFA were compared to PACS and ACS at last follow-up, arterial hypertension (65.3% vs. 81.9% and 92.0%; p<0.05), diabetes (23.8% vs. 35.6% and 40.0%; p<0.01), and thromboembolic events (PACS: HR 3.43, 95%-CI 0.89-13.29; ACS: HR 5.96, 95%-CI 1.33-26.63; p<0.05) were significantly less frequent, along with a trend towards a higher rate of cardiovascular events in case of cortisol autonomy (PACS: HR 2.23, 95%-CI 0.94-5.32; ACS: HR 2.60, 95%-CI 0.87-7.79; p=0.1). Twenty-five (12.6%) of the non-operated patients died, with higher overall mortality in PACS (HR 2.6, 95%-CI 1.0-4.7; p=0.083) and ACS (HR 4.7, 95%-CI 1.6-13.3; p<0.005) compared to NFA. In operated patients, prevalence of arterial hypertension decreased significantly (77.0% at diagnosis to 61.7% at last follow-up; p<0.05). The prevalence of cardiovascular events and mortality did not differ significantly between operated and non-operated patients, whereas thromboembolic events were significantly less frequent in the surgical treatment group.
Conclusion: Our study confirms relevant cardiovascular morbidity in patients with adrenal incidentalomas (especially those with cortisol autonomy). These patients should therefore be monitored carefully, including adequate treatment of typical cardiovascular risk factors. Adrenalectomy was associated with a significantly decreased prevalence of hypertension. However, more than 30% of patients required reclassification according to repeated dexamethasone suppression tests. Thus, cortisol autonomy should ideally be confirmed before making any relevant treatment decision (e.g. adrenalectomy).
Keywords: adrenal imaging; adrenal tumours; autonomous cortisol secretion; cardiovascular events; cardiovascular risk factors; dexamethasone suppression test; morbidity; mortality.
Copyright © 2023 Remde, Kranz, Morell, Altieri, Kroiss, Detomas, Fassnacht and Deutschbein.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Fassnacht M, Arlt W, Bancos I, Dralle H, Newell-Price J, Sahdev A, et al. Management of adrenal incidentalomas: European society of endocrinology clinical practice guideline in collaboration with the European network for the study of adrenal tumors. Eur J Endocrinol (2016) 175(2):G1–G34. doi: 10.1530/EJE-16-0467 - DOI - PubMed
-
- Deutschbein T, Reimondo G, Di Dalmazi G, Bancos I, Patrova J, Vassiliadi DA, et al. Age-dependent and sex-dependent disparity in mortality in patients with adrenal incidentalomas and autonomous cortisol secretion: An international, retrospective, cohort study. Lancet Diabetes Endocrinol (2022) 10(7):499–508. doi: 10.1016/s2213-8587(22)00100-0 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical