

Candida: The Ruthless Opportunist
- PMID: 37223187
- PMCID: PMC10201639
- DOI: 10.7759/cureus.37969
Candida: The Ruthless Opportunist
Abstract
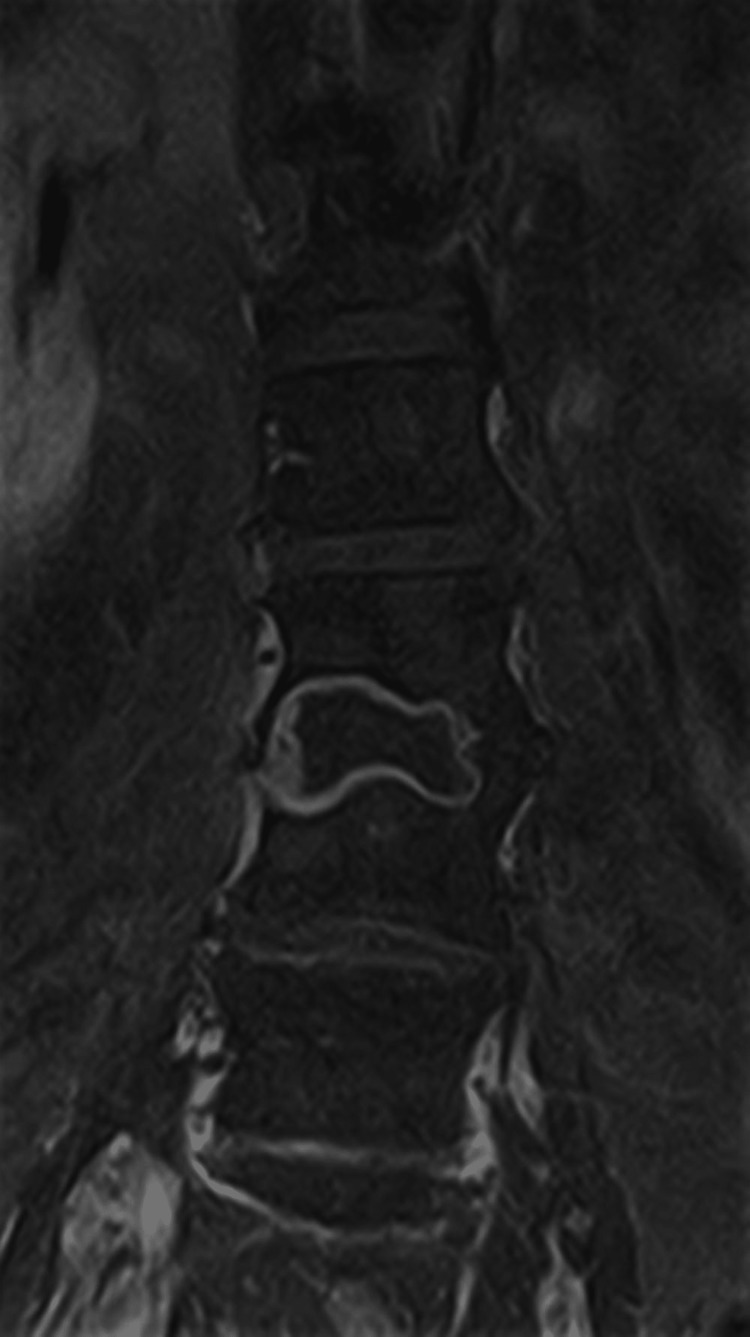
Spondylodiscitis is a pathology with a devastating potential for functional limitation in patients, which may involve immobilization for months due to the risk of compression or even spinal cord section. It is a rare type of infection occurring in the vertebrae and discs of the spine, and most are bacterial. Fungal cases are rare. We present the clinical case of a 52-year-old female patient with a past medical history of vesicular lithiasis and degenerative disc disease of the cervical spine and no home medication. The patient was hospitalized in the surgery service for about 3.5 months due to necro-hemorrhagic lithiasic pancreatitis that evolved into septic shock and needed organ support in intensive care for 2.5 weeks. Several cycles of antibiotics and endoscopic retrograde cholangiopancreatography (ERCP) with stent placement were performed. She was readmitted for urgent care to the hospital of residence with fever, sweating, and low back pain with sciatica five days after discharge. Lumbar CT and MRI evidence showed the destruction of about two-thirds of the vertebral bodies L3-L4, L5-S1, and adjacent discs, pointing to the diagnosis of infectious spondylodiscitis. Candida albicans was found in blood cultures and lumbar biopsies. The patient was treated with oral fluconazole 400 mg/day for eight months, and the control MRIs showed slow but favorable bone sclerosis over time. She spent a total of 13.5 months in the hospital, including five months in bedbound status. The patient left the hospital walking without any assistance, with an upright mood and disposition. The most likely main fungal infectious factors were the manipulation of the bile ducts, immunosuppression associated with corticosteroid therapy, and multiorgan septic failure. The authors highlight this clinical case for its rarity, complications leading to candidemia, diagnostic and therapeutic delay, complexity, and risk of irreversible injuries to which the patient was subjected. The total recuperation of the patient after such a long physical and emotional struggle was very gratifying.
Keywords: antifungal; candida; candida infections; endoscopic retrograde cholangiopancreatography; fungi; lithiasic pancreatitis; magnetic resonance imaging; sepsis; spondylodiscitis.
Copyright © 2023, Rebolo et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures





References
-
- The epidemiology of vertebral osteomyelitis in the United States from 1998 to 2013 . Issa K, Diebo BG, Faloon M, Naziri Q, Pourtaheri S, Paulino CB, Emami A. https://doi.org/10.1097/BSD.0000000000000597 Clin Spine Surg. 2018;31:0–8. - PubMed
-
- 2015 Infectious Diseases Society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of Native vertebral osteomyelitis in adults. Berbari EF, Kanj SS, Kowalski TJ, et al. https://doi.org/10.1093/cid/civ482 Clin Infect Dis. 2015;61:0–46. - PubMed
-
- Incidence and risk factors for mortality of vertebral osteomyelitis: a retrospective analysis using the Japanese diagnosis procedure combination database. Akiyama T, Chikuda H, Yasunaga H, Horiguchi H, Fushimi K, Saita K. https://doi.org/10.1136/bmjopen-2012-002412 BMJ Open. 2013;3:0. - PMC - PubMed
-
- Long-term outcome of pyogenic vertebral osteomyelitis: a cohort study of 260 patients. Gupta A, Kowalski TJ, Osmon DR, et al. https://doi.org/10.1093/ofid/ofu107 Open Forum Infect Dis. 2014;1:0. - PMC - PubMed
-
- Predicting patients with concurrent noncontiguous spinal epidural abscess lesions. Ju KL, Kim SD, Melikian R, Bono CM, Harris MB. https://doi.org/10.1016/j.spinee.2014.06.008. Spine J. 2015;15:95–101. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous