

Comparing In-Hospital Mortality Prediction by Senior Emergency Resident's Judgment and Prognostic Models in the Emergency Department
- PMID: 37223337
- PMCID: PMC10202605
- DOI: 10.1155/2023/6042762
Comparing In-Hospital Mortality Prediction by Senior Emergency Resident's Judgment and Prognostic Models in the Emergency Department
Abstract
Background: A comparison of emergency residents' judgments and two derivatives of the Sequential Organ Failure Assessment (SOFA), namely, the mSOFA and the qSOFA, was conducted to determine the accuracy of predicting in-hospital mortality among critically ill patients in the emergency department (ED).
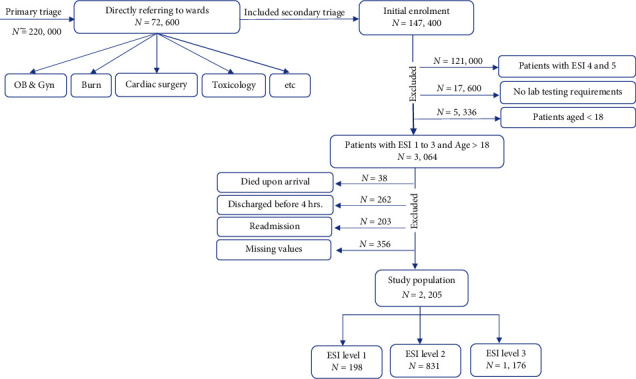
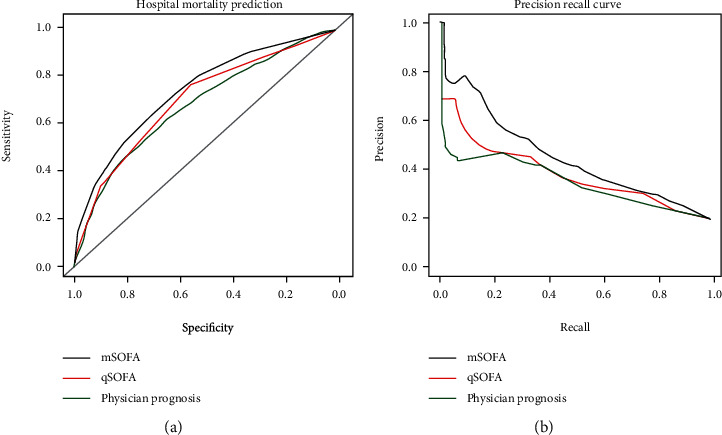
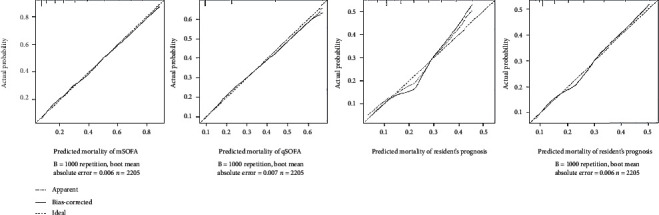
Methods: A prospective cohort research was performed on patients over 18 years of age presented to the ED. We used logistic regression to develop a model for predicting in-hospital mortality by using qSOFA, mSOFA, and residents' judgment scores. We compared the accuracy of prognostic models and residents' judgment in terms of the overall accuracy of the predicted probabilities (Brier score), discrimination (area under the ROC curve), and calibration (calibration graph). Analyses were carried out using R software version R-4.2.0.
Results: In the study, 2,205 patients with median age of 64 (IQR: 50-77) years were included. There were no significant differences between the qSOFA (AUC 0.70; 95% CI: 0.67-0.73) and physician's judgment (AUC 0.68; 0.65-0.71). Despite this, the discrimination of mSOFA (AUC 0.74; 0.71-0.77) was significantly higher than that of the qSOFA and residents' judgments. Additionally, the AUC-PR of mSOFA, qSOFA, and emergency resident's judgments was 0.45 (0.43-0.47), 0.38 (0.36-0.40), and 0.35 (0.33-0.37), respectively. The mSOFA appears stronger in terms of overall performance: 0.13 vs. 0.14 and 0.15. All three models showed good calibration.
Conclusion: The performance of emergency residents' judgment and the qSOFA was the same in predicting in-hospital mortality. However, the mSOFA predicted better-calibrated mortality risk. Large-scale studies should be conducted to determine the utility of these models.
Copyright © 2023 Zahra Rahmatinejad et al.
Conflict of interest statement
There is no conflict of interest to declare.
Figures
References
-
- Rahmatinejad Z., Rahmatinejad F., Sezavar M., Tohidinezhad F., Abu-Hanna A., Eslami S. Internal validation and evaluation of the predictive performance of models based on the PRISM-3 (Pediatric Risk of Mortality) and PIM-3 (Pediatric Index of Mortality) scoring systems for predicting mortality in Pediatric Intensive Care Units (PICUs) BMC Pediatrics . 2022;22(1):p. 199. doi: 10.1186/s12887-022-03228-y. - DOI - PMC - PubMed
-
- Yarmohammadian M. H., Rezaei F., Haghshenas A., Tavakoli N. Overcrowding in emergency departments: a review of strategies to decrease future challenges. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences . 2017;22(1):p. 23. doi: 10.4103/1735-1995.200277. - DOI - PMC - PubMed
-
- Goshayeshi L., Akbari Rad M., Bergquist R., Allahyari A., Hashemzadeh K., Hoseini B. Demographic and clinical characteristics of severe Covid-19 infections: a cross-sectional study from Mashhad University of Medical Sciences, Iran. BMC Infectious Diseases . 2021;21(1):p. 656. doi: 10.1186/s12879-021-06363-6. - DOI - PMC - PubMed
-
- Khodashahi R., Naderi H. R., Sedaghat A., et al. Intravenous immunoglobulin for treatment of patients with COVID-19: a case-control study. Archives of Clinical Infectious Diseases . 2021;16(1, article e108068) doi: 10.5812/archcid.108068. - DOI
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
