

The role of imaging and sentinel lymph node biopsy in patients with T3b-T4b melanoma with clinically negative disease
- PMID: 37223678
- PMCID: PMC10200883
- DOI: 10.3389/fonc.2023.1143354
The role of imaging and sentinel lymph node biopsy in patients with T3b-T4b melanoma with clinically negative disease
Abstract
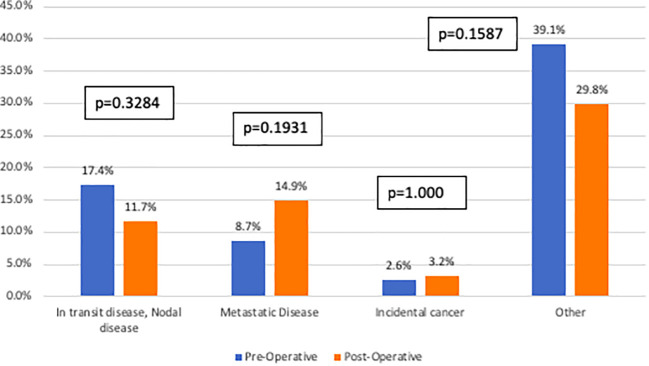
Background: Previous studies demonstrate minimal utility of pre-operative imaging for low-risk melanoma; however, imaging may be more critical for patients with high-risk disease. Our study evaluates the impact of peri-operative cross-sectional imaging in patients with T3b-T4b melanoma.
Methods: Patients with T3b-T4b melanoma who underwent wide local excision were identified from a single institution (1/1/2005 - 12/31/2020). Cross-sectional imaging was defined as body CT, PET and/or MRI in the perioperative period, with the following findings: in-transit or nodal disease, metastatic disease, incidental cancer, or other. Propensity scores were created for the odds of undergoing pre-operative imaging. Recurrence free survival was analyzed using the Kaplan-Meier method and log-rank test.
Results: A total of 209 patients were identified with a median age of 65 (IQR 54-76), of which the majority were male (65.1%), with nodular melanoma (39.7%) and T4b disease (47.9%). Overall, 55.0% underwent pre-operative imaging. There were no differences in imaging findings between the pre- and post-operative cohorts. After propensity-score matching, there was no difference in recurrence free survival. Sentinel node biopsy was performed in 77.5% patients, with 47.5% resulting in a positive result.
Conclusion: Pre-operative cross-sectional imaging does not impact the management of patients with high-risk melanoma. Careful consideration of imaging use is critical in the management of these patients and highlights the importance of sentinel node biopsy for stratification and decision making.
Keywords: cross-sectional imaging; high-risk melanoma; recurrence free survival; sentinel lymph node (SLN) biopsy; surgical management.
Copyright © 2023 Papageorge, Maina, King, Lee, Baumann, Pucar, Ariyan, Khan, Weiss, Clune and Olino.
Conflict of interest statement
The reviewer KE declared a shared affiliation with the author SW to the handling editor at the time of review. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



Similar articles
-
Sentinel lymph node biopsy in patients with clinical stage IIB/C cutaneous melanoma: A national cohort study.J Am Acad Dermatol. 2022 Oct;87(4):754-760. doi: 10.1016/j.jaad.2022.04.025. Epub 2022 Apr 22. J Am Acad Dermatol. 2022. PMID: 35469980
-
Active surveillance of patients who have sentinel node positive melanoma: An international, multi-institution evaluation of adoption and early outcomes after the Multicenter Selective Lymphadenectomy Trial II (MSLT-2).Cancer. 2021 Jul 1;127(13):2251-2261. doi: 10.1002/cncr.33483. Epub 2021 Apr 7. Cancer. 2021. PMID: 33826754 Free PMC article.
-
Patterns of initial recurrence and prognosis after sentinel lymph node biopsy and selective lymphadenectomy for melanoma.Plast Reconstr Surg. 2003 Aug;112(2):486-97. doi: 10.1097/01.PRS.0000070989.23469.1F. Plast Reconstr Surg. 2003. PMID: 12900606
-
Sentinel lymph node biopsy in patients with primary cutaneous melanoma: study of 455 cases.J Eur Acad Dermatol Venereol. 2000 Jan;14(1):35-45. doi: 10.1046/j.1468-3083.2000.00005.x. J Eur Acad Dermatol Venereol. 2000. PMID: 10877250 Review.
-
Adjuvant therapy of malignant melanoma and the role of sentinel node mapping.Recent Results Cancer Res. 2000;157:178-89. doi: 10.1007/978-3-642-57151-0_15. Recent Results Cancer Res. 2000. PMID: 10857171 Review.
Cited by
-
Management of melanoma: can we use gene expression profiling to help guide treatment and surveillance?Clin Exp Metastasis. 2024 Aug;41(4):439-445. doi: 10.1007/s10585-023-10241-7. Epub 2023 Dec 8. Clin Exp Metastasis. 2024. PMID: 38064126 Review.
References
-
- Survival rates for melanoma skin cancer (2022). Available at: https://www.cancer.org/cancer/melanoma-skin-cancer/detection-diagnosis-s....
-
- Luke JJ, Rutkowski P, Queirolo P, Del Vecchio M, Mackiewicz J, Chiarion-Sileni V, et al. . Pembrolizumab versus placebo as adjuvant therapy in completely resected stage IIB or IIC melanoma (KEYNOTE-716): a randomised, double-blind, phase 3 trial. Lancet (2022) 399(10336):1718–29. doi: 10.1016/S0140-6736(22)00562-1 - DOI - PubMed
LinkOut - more resources
Full Text Sources