

doi: 10.1016/j.xfre.2023.02.002.
eCollection 2023 Jun.
Clinical development of the oral gonadotropin-releasing hormone antagonist elagolix
Affiliations
- PMID: 37223767
- PMCID: PMC10201304
- DOI: 10.1016/j.xfre.2023.02.002
Item in Clipboard
Clinical development of the oral gonadotropin-releasing hormone antagonist elagolix
F S Rep.
.
Abstract
Elagolix is the first oral gonadotropin-releasing hormone antagonist that entered clinical development and received regulatory approval for the management of women with endometriosis and heavy menstrual bleeding associated with uterine fibroids in combination with a hormonal add-back therapy. This mini review aims to summarize the key clinical studies that led to its regulatory approval.
Keywords: Elagolix; GnRH antagonist; endometriosis; uterine fibroids.
© 2023 The Author.
Figures
Elagolix. (From Taylor et al. [5]. Reprinted by permission of the publisher.)
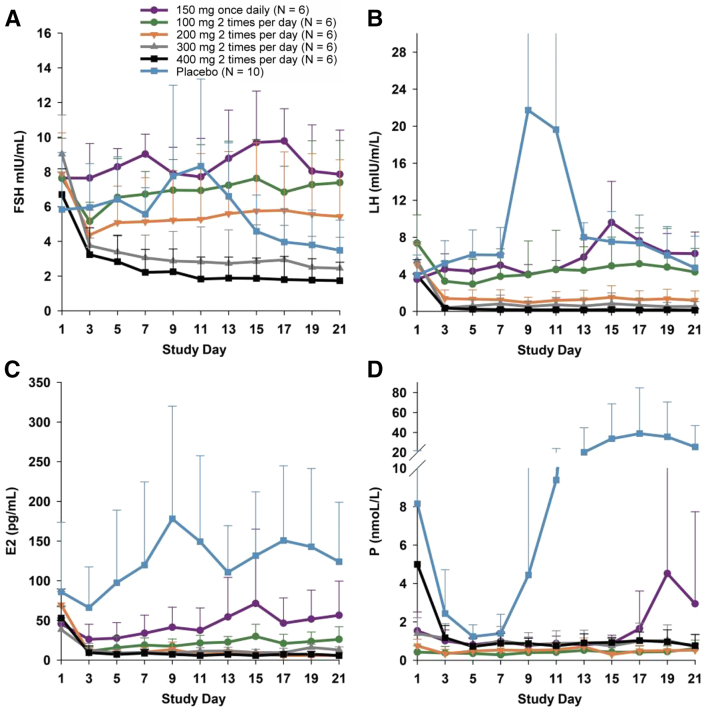
Dose-dependent suppression of gonadotropins (luteinizing hormone [LH], follicle-stimulating hormone [FSH]), estradiol (E2), and progesterone (P) in healthy premenopausal women. Concentrations (means ± SD) of (A) FSH, (B) LH, (C) E2, and (D) P during 21 days of dosing with placebo or elagolix. For the placebo group, the error bars for some time points have been truncated. (From Ng et al. [1]. Reprinted by permission of the publisher.)
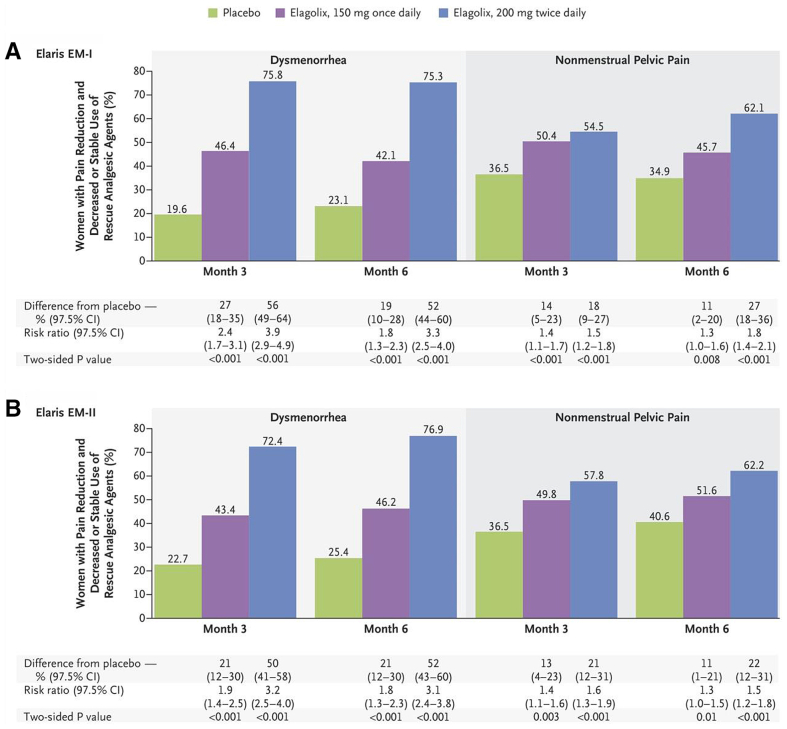
Reduction in dysmenorrhea and nonmenstrual pelvic pain during treatment with elagolix in women with endometriosis-associated pain (Elaris EM-I and EM-II studies). The percentages of women in whom the 2 primary end points (clinically meaningful reduction in dysmenorrhea or in nonmenstrual pelvic pain, as measured by the decreased or stable use of rescue analgesic agents) were reported at 3 and 6 months in (A) Elaris EM-I and (B) Elaris EM-II. In Elaris EM-I, 3-month data were provided for 373 women who received placebo, 248 who received the lower elagolix dose (150 mg once daily), and 244 who received the higher elagolix dose (200 mg twice daily); the corresponding 6-month data were provided for 372, 247, and 243 women. In Elaris EM-II, 3-month data were provided for 353 women who received placebo, 221 who received the lower elagolix dose, and 225 who received the higher elagolix dose; the corresponding 6-month data were provided for 355, 221, and 225 women. EM = endometriosis; CI = confidence interval. (From Taylor et al. [6]. Reprinted by permission of the publisher.)
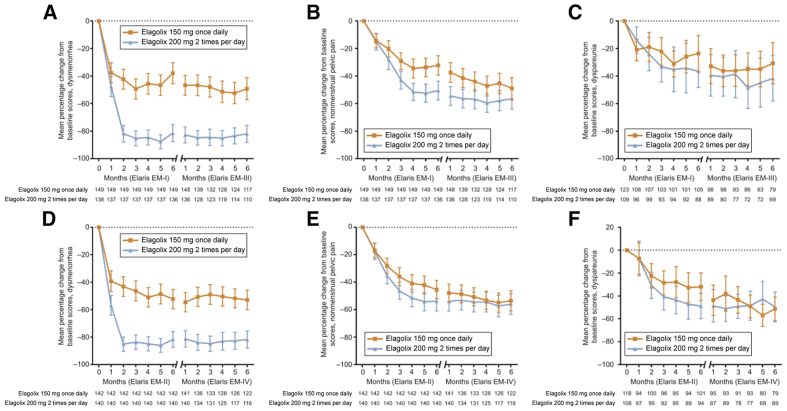
Mean percentage change from baseline in the dysmenorrhea, nonmenstrual pelvic, and dyspareunia pain scores during the long-term treatment with elagolix in women with endometriosis-associated pain (Elaris EM-III and EM-IV studies). Mean percentage change from baseline in the (A and D) dysmenorrhea, (B and E) nonmenstrual pelvic pain, and (C and F) dyspareunia scores. Error bars represent 95% confidence intervals. Between-group comparisons were not predefined and not performed. Months 1–6 in Elaris EM-I and Elaris EM-II were from women who enrolled in the extension studies Elaris EM-II and Elaris EM-IV. EM = endometriosis. (From Surrey et al. [7]. Reprinted by permission of the publisher.)
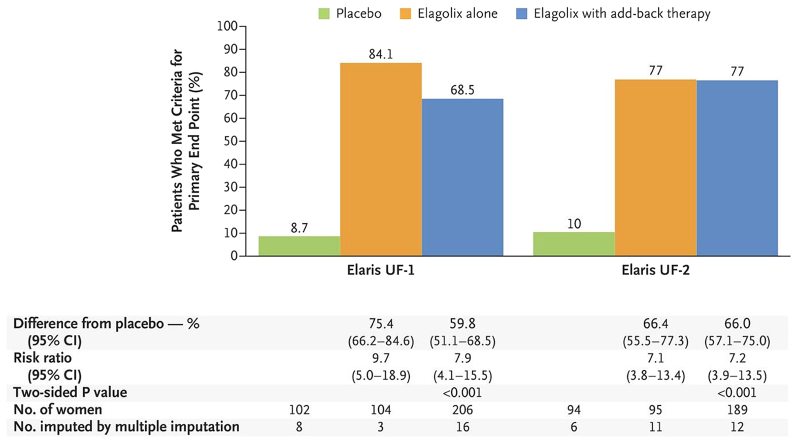
Reduction in heavy menstrual bleeding in women with uterine fibroids. The percentages of women who met the criteria for the primary end point (a menstrual blood loss volume of <80 mL in the final month and a >50% reduction in the menstrual blood loss volume from baseline to the final month) in the 2 trials. A significantly greater percentage of women who received elagolix with add-back therapy met the criteria for the primary end point than women who received placebo. The final month was defined as the last 28 days before and including the last treatment period visit date. CI = confidence interval. (From Schlaff et al. [11]. Reprinted by permission of the publisher.)
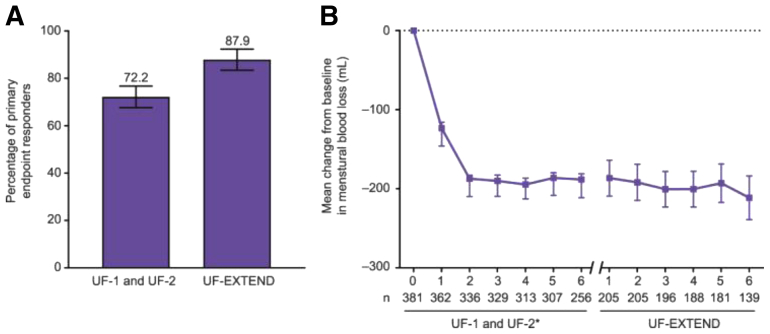
Reduction in heavy menstrual bleeding in women with uterine fibroids during long-term treatment. Percentage of women who met (A) the primary end point and (B) mean change from baseline in menstrual blood loss in women treated with up to 12 months of elagolix with add-back therapy. Data are % or mean with error bars indicating 95% confidence interval. Baseline was before first dosing in the Elaris Uterine Fibroids 1 (UF-1) and 2 (UF-2) studies. ∗The mean changes from baseline in menstrual blood loss for UF-1 and UF-2 are presented as least squares means. (From Simon et al. [12]. Reprinted by permission of the publisher.)
References
-
- Ng J., Chwalisz K., Carter D.C., Klein C.E. Dose-dependent suppression of gonadotropins and ovarian hormones by elagolix in healthy premenopausal women. J Clin Endocrinol Metab. 2017;102:1683–1691. - PubMed
-
- Millar R.P., Zhu Y.F., Chen C., Struthers R.S. Progress towards the development of non-peptide orally-active gonadotropin-releasing hormone (GnRH) antagonists: therapeutic implications. Br Med Bull. 2000;56:761–772. - PubMed
-
- Tucci F.C., Zhu Y.F., Struthers R.S., Guo Z., Gross T.D., Rowbottom M.W., et al. 3-[(2R)-amino-2-phenylethyl]-1-(2,6-difluorobenzyl)-5-(2-fluoro-3-methoxyphenyl)- 6-methylpyrimidin-2,4-dione (NBI 42902) as a potent and orally active antagonist of the human gonadotropin-releasing hormone receptor. Design, synthesis, and in vitro and in vivo characterization. J Med Chem. 2005;48:1169–1178. - PubMed
-
- Chen C., Wu D., Guo Z., Xie Q., Reinhart G.J., Madan A., et al. Discovery of sodium R-(+)-4-{2-[5-(2-fluoro-3-methoxyphenyl)-3-(2-fluoro-6-[trifluoromethyl]benzyl)-4-methyl-2,6-dioxo-3,6-dihydro-2H-pyrimidin-1-yl]-1-phenylethylamino}butyrate (elagolix), a potent and orally available nonpeptide antagonist of the human gonadotropin-releasing hormone receptor. J Med Chem. 2008;51:7478–7485. - PubMed
-
- Taylor H.S., Dun E.C., Chwalisz K. Clinical evaluation of the oral gonadotropin-releasing hormone-antagonist elagolix for the management of endometriosis-associated pain. Pain Manag. 2019;9:497–515. - PubMed
LinkOut - more resources
Full Text Sources
