

Heterogeneity of Lipoprotein(a) Levels Among Hispanic or Latino Individuals Residing in the US
- PMID: 37223894
- PMCID: PMC10209825
- DOI: 10.1001/jamacardio.2023.1134
Heterogeneity of Lipoprotein(a) Levels Among Hispanic or Latino Individuals Residing in the US
Abstract
Importance: Lipoprotein(a) (Lp[a]) is a genetically determined risk-enhancing factor for atherosclerotic cardiovascular disease (ASCVD). The Lp(a) distribution among the diverse Hispanic or Latino community residing in the US has not been previously described, to the authors' knowledge.
Objective: To determine the distribution of Lp(a) levels across a large cohort of diverse Hispanic or Latino adults living in the US and by key demographic groups.
Design, setting, and participants: The Hispanic Community Health Study/Study of Latinos (HCHS/SOL) is a prospective, population-based, cohort study of diverse Hispanic or Latino adults living in the US. At screening, participants aged 18 to 74 years were recruited between 2008 and 2011 from 4 US metropolitan areas (Bronx, New York; Chicago, Illinois; Miami, Florida; San Diego, California). HCHS/SOL included 16 415 noninstitutionalized adults recruited through probability sampling of randomly selected households. The study population represents Hispanic or Latino participants from diverse self-identified geographic and cultural backgrounds: Central American, Cuban, Dominican, Mexican, Puerto Rican, and South American. This study evaluated a subset of HCHS/SOL participants who underwent Lp(a) measurement. Sampling weights and surveys methods were used to account for HCHS/SOL sampling design. Data for this study were analyzed from April 2021 to April 2023.
Exposure: Lp(a) molar concentration was measured by a particle-enhanced turbidimetric assay with minimized sensitivity to apolipoprotein(a) size variation.
Main outcome and measure: Lp(a) quintiles were compared using analysis of variance among key demographic groups, including self-identified Hispanic or Latino background. Median percentage genetic ancestry (Amerindian, European, West African) were compared across Lp(a) quintiles.
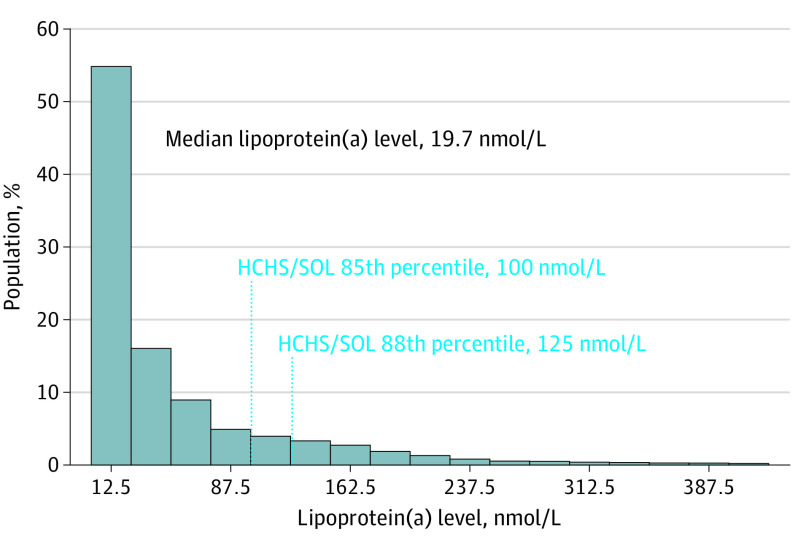
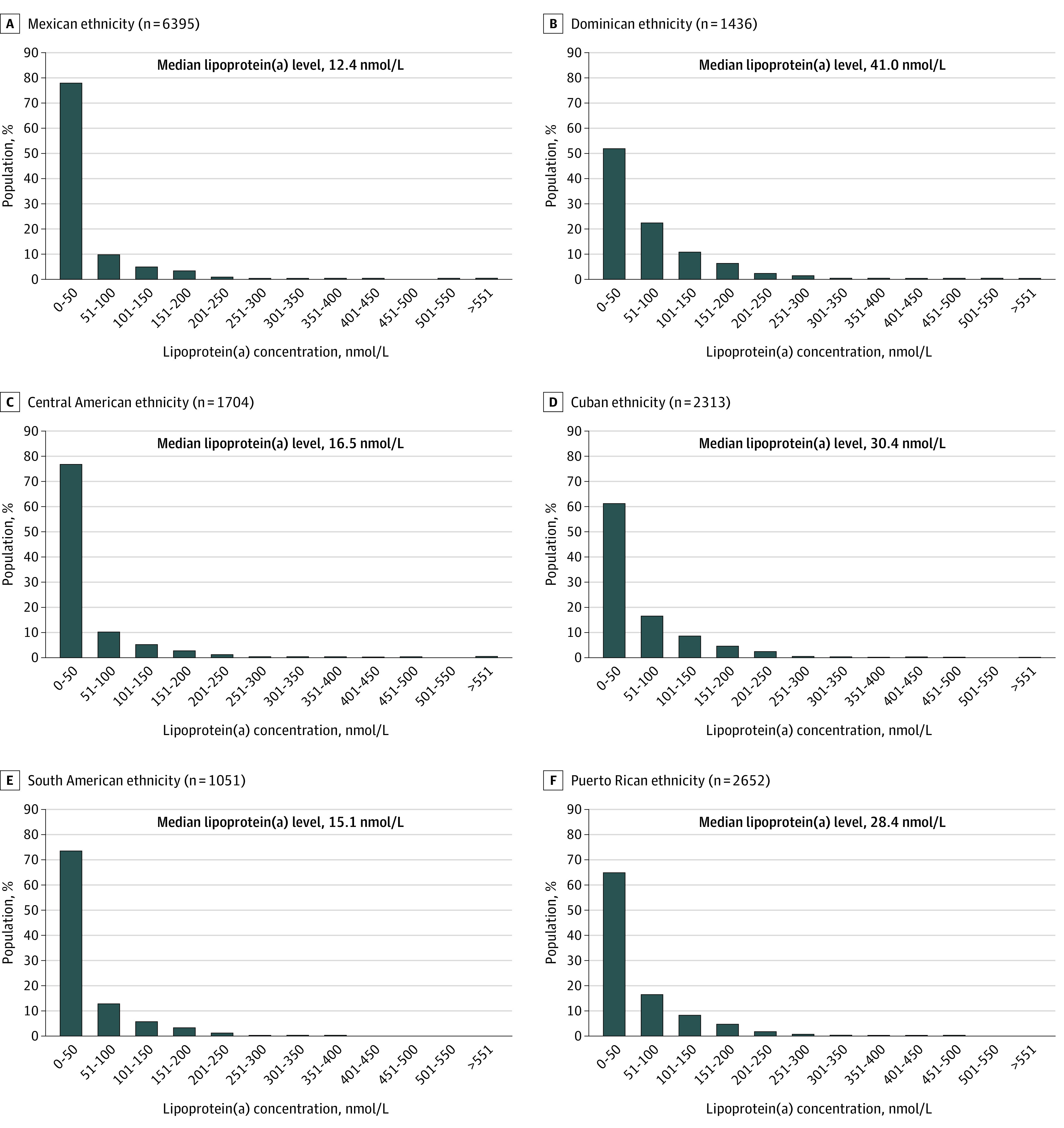
Results: Lp(a) molar concentration was measured in 16 117 participants (mean [SD] age, 41 [14.8] years; 9680 female [52%]; 1704 Central American [7.7%], 2313 Cuban [21.1%], 1436 Dominican [10.3%], 6395 Mexican [39.1%], 2652 Puerto Rican [16.6%], 1051 South American [5.1%]). Median (IQR) Lp(a) level was 19.7 (7.4-59.7) nmol/L. Across Hispanic or Latino background groups, there was significant heterogeneity in median Lp(a) levels ranging from 12 to 41 nmol/L in those reporting a Mexican vs Dominican background. Median (IQR) West African genetic ancestry was lowest in the first quintile of Lp(a) level and highest in the fifth quintile (5.5% [3.4%-12.9%] and 12.1% [5.0%-32.5%]; respectively; P < .001), whereas the converse was seen for Amerindian ancestry (32.8% [9.9%-53.2%] and 10.7% [4.9%-30.7%], respectively; P < .001).
Conclusions and relevance: Results of this cohort study suggest that differences in Lp(a) level distribution across the diverse US Hispanic or Latino population may carry important implications for the use of Lp(a) level in ASCVD risk assessment for this group. Cardiovascular outcomes data are needed to better understand the clinical impact of differences in Lp(a) levels by Hispanic or Latino background.
Conflict of interest statement
Figures
Comment in
-
When Is a High Lipoprotein (a) Concentration Too High?-The Need for Diverse Population-Based Samples.JAMA Cardiol. 2023 Jul 1;8(7):696. doi: 10.1001/jamacardio.2023.1141. JAMA Cardiol. 2023. PMID: 37223909 No abstract available.
Similar articles
-
Heterogeneity of Apolipoprotein B Levels Among Hispanic or Latino Individuals Residing in the US.JAMA Cardiol. 2025 Feb 1;10(2):164-169. doi: 10.1001/jamacardio.2024.4789. JAMA Cardiol. 2025. PMID: 39745752
-
Hearing Impairment Prevalence and Associated Risk Factors in the Hispanic Community Health Study/Study of Latinos.JAMA Otolaryngol Head Neck Surg. 2015 Jul;141(7):641-8. doi: 10.1001/jamaoto.2015.0889. JAMA Otolaryngol Head Neck Surg. 2015. PMID: 26021283 Free PMC article.
-
Cigarette Smoking and Depressive Symptoms Among Hispanic/Latino Adults: Results From the Hispanic Community Health Study/Study of Latinos (HCHS/SOL).Nicotine Tob Res. 2015 Jun;17(6):727-34. doi: 10.1093/ntr/ntu209. Epub 2014 Oct 19. Nicotine Tob Res. 2015. PMID: 25332458 Free PMC article.
-
Cardiovascular disease risk factors in the Hispanic/Latino population: lessons from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL).Prog Cardiovasc Dis. 2014 Nov-Dec;57(3):230-6. doi: 10.1016/j.pcad.2014.07.006. Epub 2014 Aug 2. Prog Cardiovasc Dis. 2014. PMID: 25242694 Review.
-
Challenges in preventing heart disease in hispanics: early lessons learned from the Hispanic Community Health Study/Study of Latinos (HCHS/SOL).Prog Cardiovasc Dis. 2014 Nov-Dec;57(3):253-61. doi: 10.1016/j.pcad.2014.08.004. Epub 2014 Aug 13. Prog Cardiovasc Dis. 2014. PMID: 25212986 Free PMC article. Review.
Cited by
-
Genetics and Pathophysiological Mechanisms of Lipoprotein(a)-Associated Cardiovascular Risk.J Am Heart Assoc. 2024 Jun 18;13(12):e033654. doi: 10.1161/JAHA.123.033654. Epub 2024 Jun 15. J Am Heart Assoc. 2024. PMID: 38879448 Free PMC article. Review.
-
Lipoprotein(a) Levels in Disaggregated Racial and Ethnic Subgroups Across Atherosclerotic Cardiovascular Disease Risk Levels.JACC Adv. 2024 May 2;3(6):100940. doi: 10.1016/j.jacadv.2024.100940. eCollection 2024 Jun. JACC Adv. 2024. PMID: 38938854 Free PMC article.
-
Association of Lp(a) With Stroke and Cerebral Injury on MRI: Insights From the HCHS/SOL (Hispanic Community Health Study/Study of Latinos) and Investigation of Neurocognitive Aging MRI (SOL-INCA MRI).Stroke. 2025 Jun;56(6):1492-1504. doi: 10.1161/STROKEAHA.124.048439. Epub 2025 Apr 1. Stroke. 2025. PMID: 40166810
-
A nomogram for predicting the risk of coronary artery disease in premenopausal women with suspected coronary artery disease.Sci Rep. 2025 Aug 11;15(1):29410. doi: 10.1038/s41598-025-14589-6. Sci Rep. 2025. PMID: 40790067 Free PMC article.
-
Advancements in genetic research by the Hispanic Community Health Study/Study of Latinos: A 10-year retrospective review.HGG Adv. 2025 Jan 9;6(1):100376. doi: 10.1016/j.xhgg.2024.100376. Epub 2024 Oct 29. HGG Adv. 2025. PMID: 39473183 Free PMC article. Review.
References
-
- Rodriguez CJ, Allison M, Daviglus ML, et al. ; American Heart Association Council on Epidemiology and Prevention; American Heart Association Council on Clinical Cardiology; American Heart Association Council on Cardiovascular and Stroke Nursing . Status of cardiovascular disease and stroke in Hispanics/Latinos in the US: a science advisory from the American Heart Association. Circulation. 2014;130(7):593-625. doi:10.1161/CIR.0000000000000071 - DOI - PMC - PubMed
-
- Reyes-Soffer G, Ginsberg HN, Berglund L, et al. ; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular Radiology and Intervention; and Council on Peripheral Vascular Disease . Lipoprotein(a): a genetically determined, causal, and prevalent risk factor for atherosclerotic cardiovascular disease: a scientific statement from the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(1):e48-e60. doi:10.1161/ATV.0000000000000147 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
