

Immunogenomic Landscape of Neuroendocrine Prostate Cancer
- PMID: 37223924
- PMCID: PMC10524949
- DOI: 10.1158/1078-0432.CCR-22-3743
Immunogenomic Landscape of Neuroendocrine Prostate Cancer
Abstract
Purpose: Patients with neuroendocrine prostate cancer (NEPC) are often managed with immunotherapy regimens extrapolated from small-cell lung cancer (SCLC). We sought to evaluate the tumor immune landscape of NEPC compared with other prostate cancer types and SCLC.
Experimental design: In this retrospective study, a cohort of 170 patients with 230 RNA-sequencing and 104 matched whole-exome sequencing data were analyzed. Differences in immune and stromal constituents, frequency of genomic alterations, and associations with outcomes were evaluated.
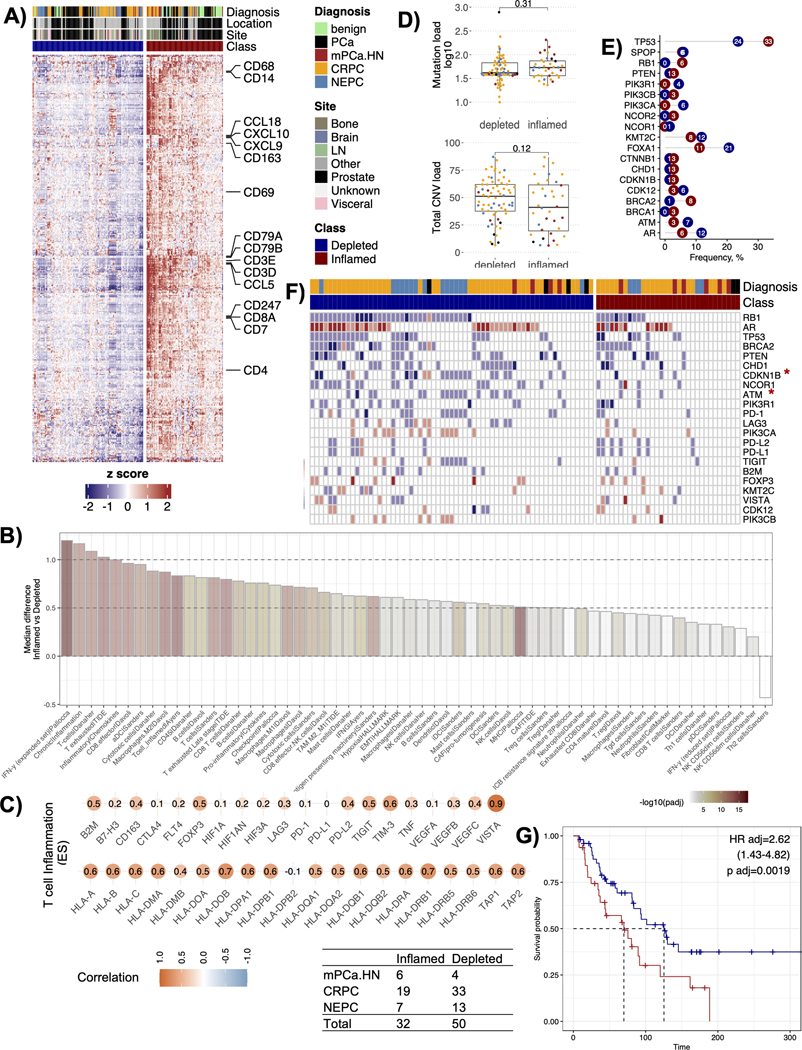
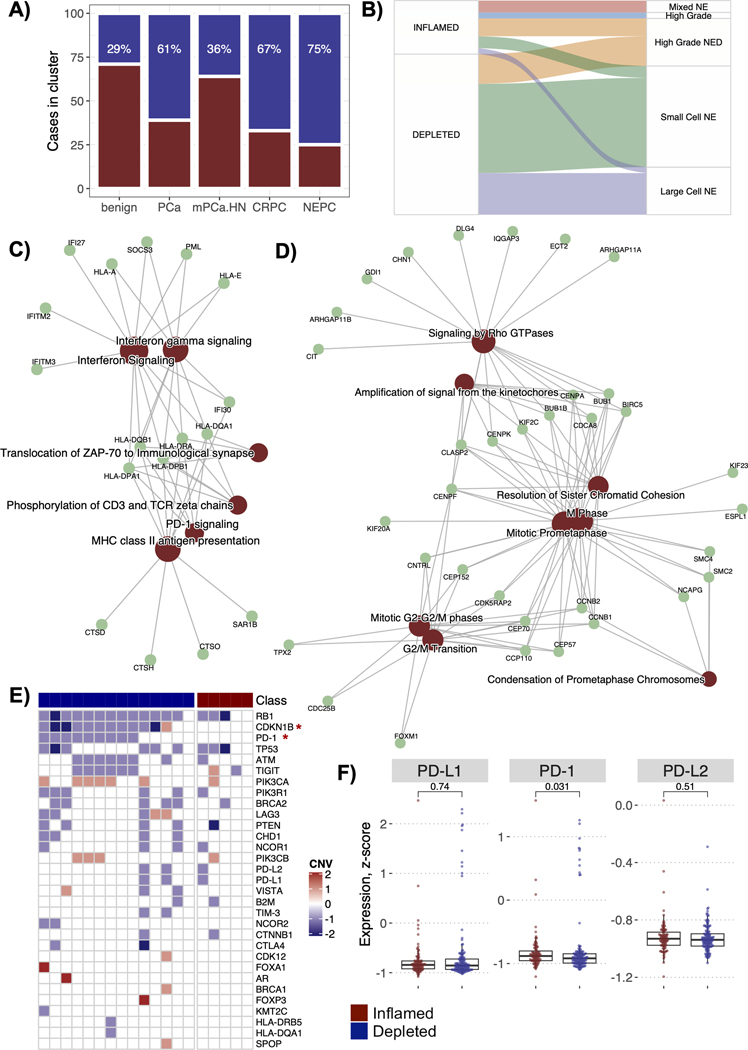
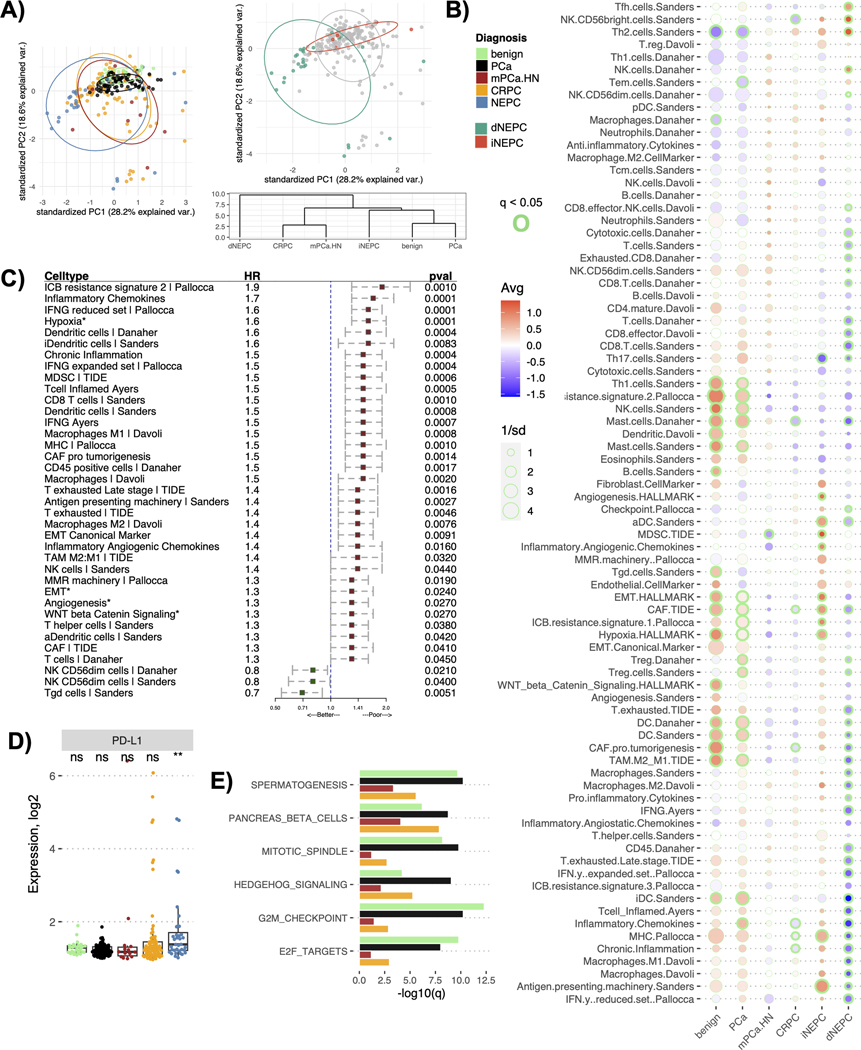
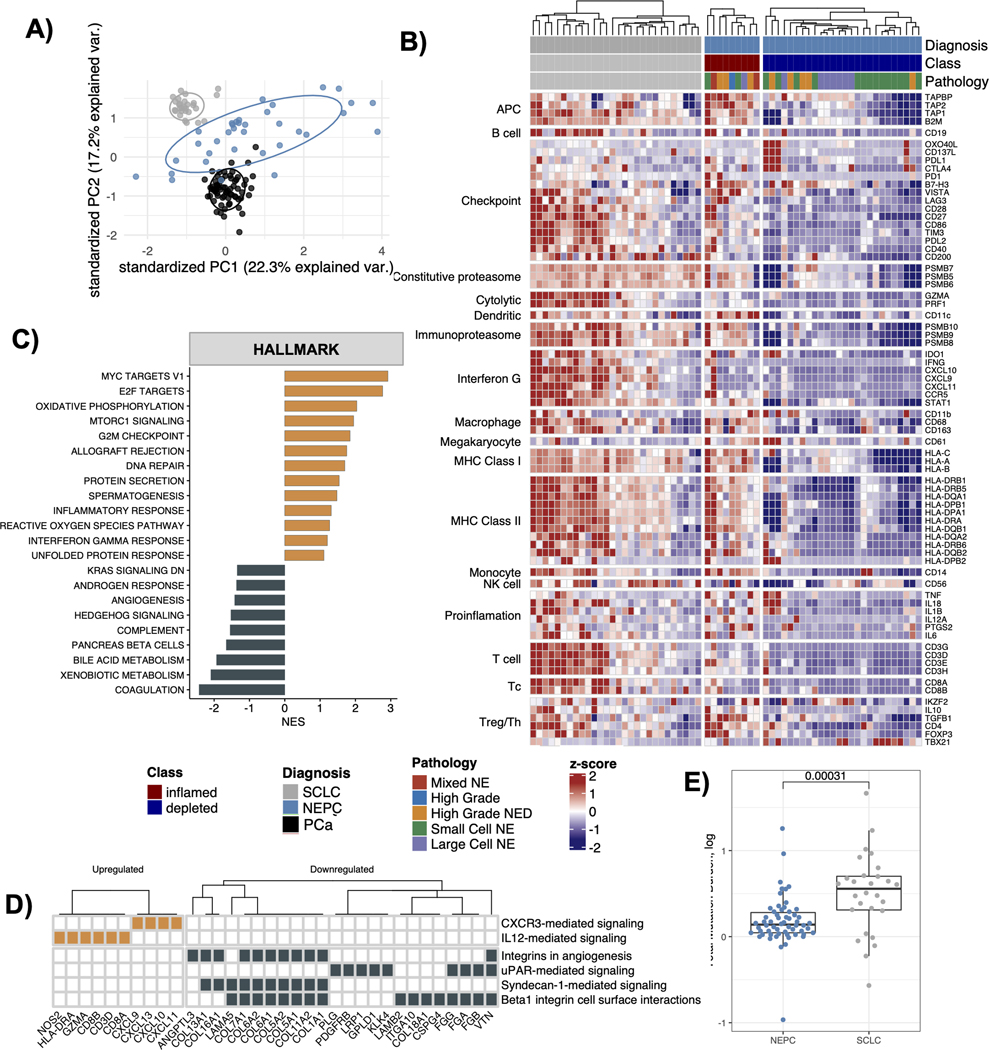
Results: In our cohort, 36% of the prostate tumors were identified as CD8+ T-cell inflamed, whereas the remaining 64% were T-cell depleted. T-cell-inflamed tumors were enriched in anti-inflammatory M2 macrophages and exhausted T cells and associated with shorter overall survival relative to T-cell-depleted tumors (HR, 2.62; P < 0.05). Among all prostate cancer types in the cohort, NEPC was identified to be the most immune depleted, wherein only 9 out of the 36 total NEPC tumors were classified as T-cell inflamed. These inflamed NEPC cases were enriched in IFN gamma signaling and PD-1 signaling compared with other NEPC tumors. Comparison of NEPC with SCLC revealed that NEPC had poor immune content and less mutations compared with SCLC, but expression of checkpoint genes PD-L1 and CTLA-4 was comparable between NEPC and SCLC.
Conclusions: NEPC is characterized by a relatively immune-depleted tumor immune microenvironment compared with other primary and metastatic prostate adenocarcinoma except in a minority of cases. These findings may inform development of immunotherapy strategies for patients with advanced prostate cancer.
©2023 American Association for Cancer Research.
Conflict of interest statement
H.B. has served as consultant/advisory board member for Janssen, Astellas, Merck, Pfizer, Foundation Medicine, Blue Earth Diagnostics, Amgen, Bayer, Oncorus, LOXO, Daicchi Sankyo, Sanofi, Curie Therapeutics, Novartis, Astra Zeneca; H.B. has received research funding from Janssen, AbbVie/Stemcentrx, Eli Lilly, Astellas, Millennium, Bristol Myers Squibb, Circle Pharma, Daicchi Sankyo, Novartis. O.E. is supported by Janssen, J&J, Astra-Zeneca, Volastra and Eli Lilly research grants; O.E. is scientific advisor and equity holder in Freenome, Owkin, Pionyr Immunotherapeutics, Volastra Therapeutics and One Three Biotech and a paid scientific advisor to Champions Oncology; V.C. has served as a consultant/advisory board member for Janssen, Astellas, Merck, AstraZeneca, Amgen, and Bayer; V.C. has received speaker honoraria or travel support from Astellas, Janssen, Ipsen, Bayer and Bristol.
Figures
References
-
- Sung H, et al., Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin, 2021. 71(3): p. 209–249. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
