

Gene expression signature predicts rate of type 1 diabetes progression
- PMID: 37224769
- PMCID: PMC10277927
- DOI: 10.1016/j.ebiom.2023.104625
Gene expression signature predicts rate of type 1 diabetes progression
Abstract
Background: Type 1 diabetes is a complex heterogenous autoimmune disease without therapeutic interventions available to prevent or reverse the disease. This study aimed to identify transcriptional changes associated with the disease progression in patients with recent-onset type 1 diabetes.
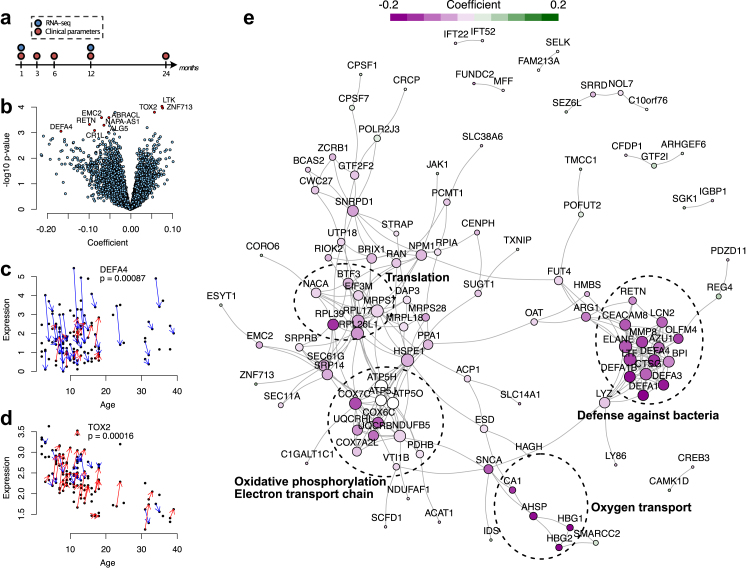
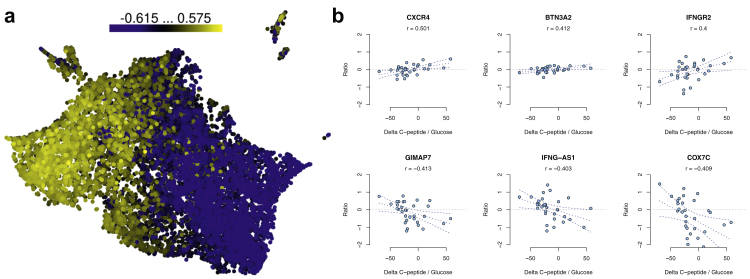
Methods: Whole-blood samples were collected as part of the INNODIA study at baseline and 12 months after diagnosis of type 1 diabetes. We used linear mixed-effects modelling on RNA-seq data to identify genes associated with age, sex, or disease progression. Cell-type proportions were estimated from the RNA-seq data using computational deconvolution. Associations to clinical variables were estimated using Pearson's or point-biserial correlation for continuous and dichotomous variables, respectively, using only complete pairs of observations.
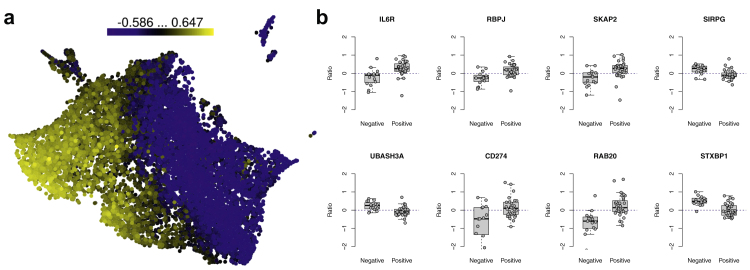
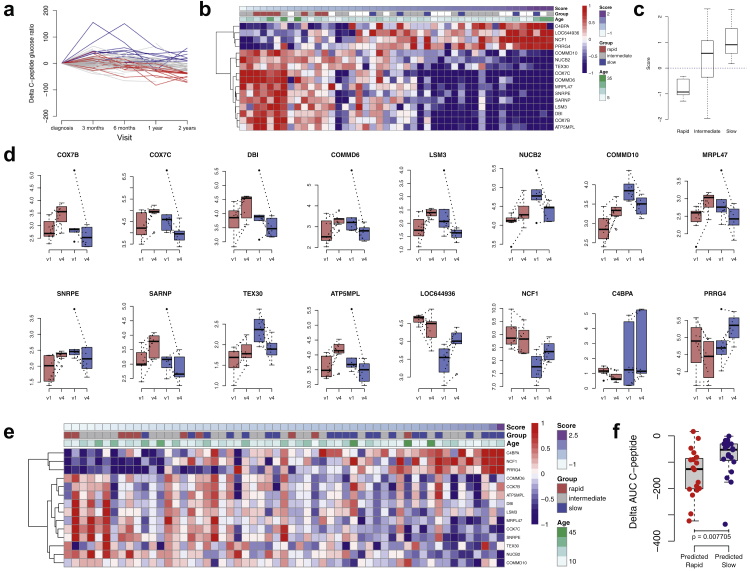
Findings: We found that genes and pathways related to innate immunity were downregulated during the first year after diagnosis. Significant associations of the gene expression changes were found with ZnT8A autoantibody positivity. Rate of change in the expression of 16 genes between baseline and 12 months was found to predict the decline in C-peptide at 24 months. Interestingly and consistent with earlier reports, increased B cell levels and decreased neutrophil levels were associated with the rapid progression.
Interpretation: There is considerable individual variation in the rate of progression from appearance of type 1 diabetes-specific autoantibodies to clinical disease. Patient stratification and prediction of disease progression can help in developing more personalised therapeutic strategies for different disease endotypes.
Funding: A full list of funding bodies can be found under Acknowledgments.
Keywords: Autoantibodies; Gene expression signature; Predictive model; RNA-seq; Type 1 diabetes.
Copyright © 2023 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests CM serves or has served on the advisory panel for ActoBio Therapeutics, AstraZeneca, Avotres, Boehringer Ingelheim, Eli Lilly and Company, Imcyse, Insulet, Mannkind, Medtronic, Merck Sharp and Dohme Ltd., Novartis, Novo Nordisk, Pfizer, Roche, Sandoz, Sanofi, Vertex, and Zealand Pharma. CM serves or has served on the speakers bureau for AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, Novartis, Novo Nordisk, and Sanofi. “T.G. was supported by Academy of Finland, Tampere University and University of Turku”.
Figures
References
-
- Ziegler A.-G., Bonifacio E., BABYDIAB-BABYDIET Study Group Age-related islet autoantibody incidence in offspring of patients with type 1 diabetes. Diabetologia. 2012;55:1937–1943. - PubMed
