

Early autoimmunity and outcome in virus encephalitis: a retrospective study based on tissue-based assay
- PMID: 37225405
- PMCID: PMC10359542
- DOI: 10.1136/jnnp-2022-330626
Early autoimmunity and outcome in virus encephalitis: a retrospective study based on tissue-based assay
Abstract
To explore the autoimmune response and outcome in the central nervous system (CNS) at the onset of viral infection and correlation between autoantibodies and viruses.
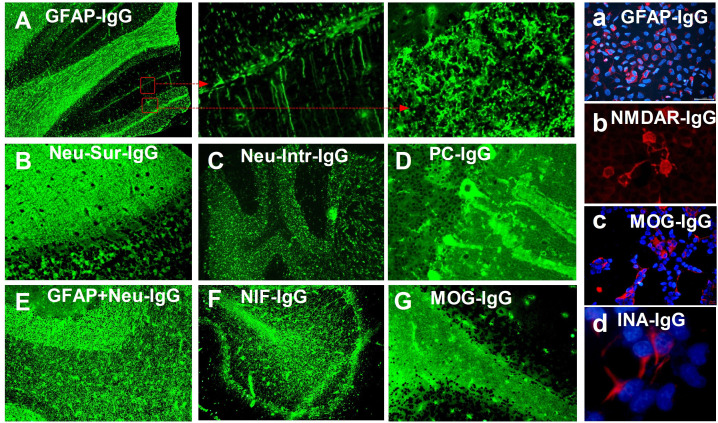
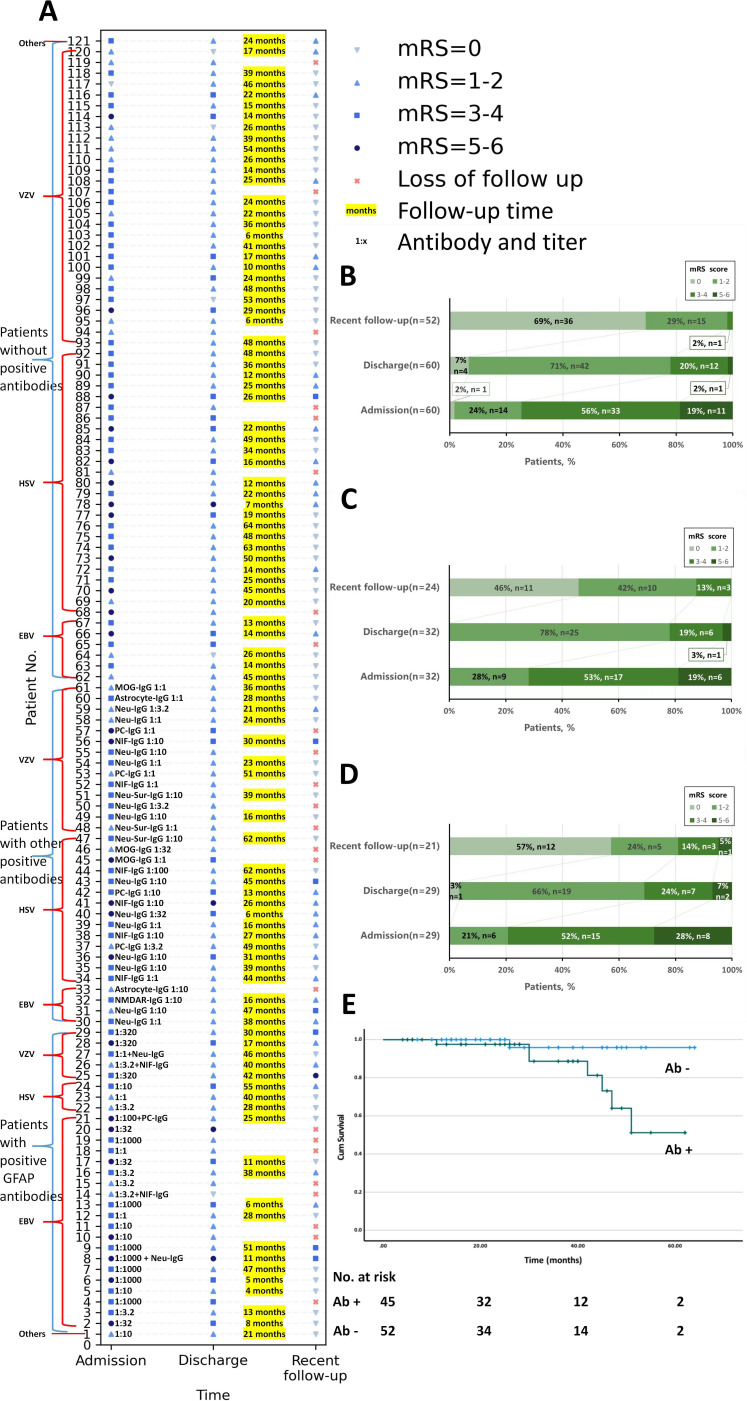
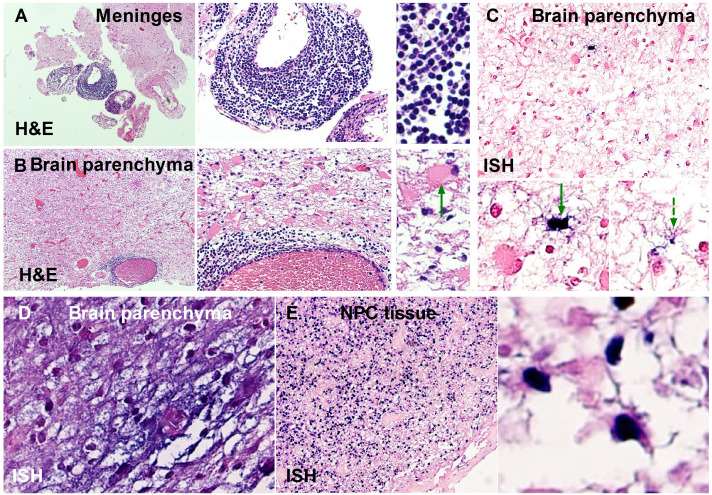
Methods: A retrospective observational study was conducted in 121 patients (2016-2021) with a CNS viral infection confirmed via cerebrospinal fluid (CSF) next-generation sequencing (cohort A). Their clinical information was analysed and CSF samples were screened for autoantibodies against monkey cerebellum by tissue-based assay. In situ hybridisation was used to detect Epstein-Barr virus (EBV) in brain tissue of 8 patients with glial fibrillar acidic protein (GFAP)-IgG and nasopharyngeal carcinoma tissue of 2 patients with GFAP-IgG as control (cohort B).
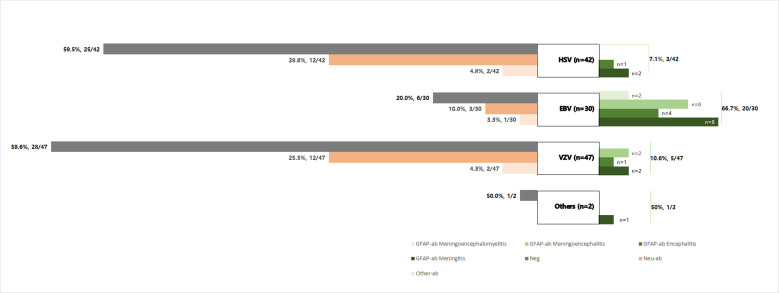
Results: Among cohort A (male:female=79:42; median age: 42 (14-78) years old), 61 (50.4%) participants had detectable autoantibodies in CSF. Compared with other viruses, EBV increased the odds of having GFAP-IgG (OR 18.22, 95% CI 6.54 to 50.77, p<0.001). In cohort B, EBV was found in the brain tissue from two of eight (25.0%) patients with GFAP-IgG. Autoantibody-positive patients had a higher CSF protein level (median: 1126.00 (281.00-5352.00) vs 700.00 (76.70-2899.00), p<0.001), lower CSF chloride level (mean: 119.80±6.24 vs 122.84±5.26, p=0.005), lower ratios of CSF-glucose/serum-glucose (median: 0.50[0.13-0.94] vs 0.60[0.26-1.23], p=0.003), more meningitis (26/61 (42.6%) vs 12/60 (20.0%), p=0.007) and higher follow-up modified Rankin Scale scores (1 (0-6) vs 0 (0-3), p=0.037) compared with antibody-negative patients. A Kaplan-Meier analysis revealed that autoantibody-positive patients experienced significantly worse outcomes (p=0.031).
Conclusions: Autoimmune responses are found at the onset of viral encephalitis. EBV in the CNS increases the risk for autoimmunity to GFAP.
Keywords: autoimmune encephalitis; clinical neurology; neuroimmunology; neurovirology.
© Author(s) (or their employer(s)) 2023. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous