

Partial splenic embolization as a rescue and emergency treatment for portal hypertension and gastroesophageal variceal hemorrhage
- PMID: 37226088
- PMCID: PMC10207732
- DOI: 10.1186/s12876-023-02808-1
Partial splenic embolization as a rescue and emergency treatment for portal hypertension and gastroesophageal variceal hemorrhage
Abstract
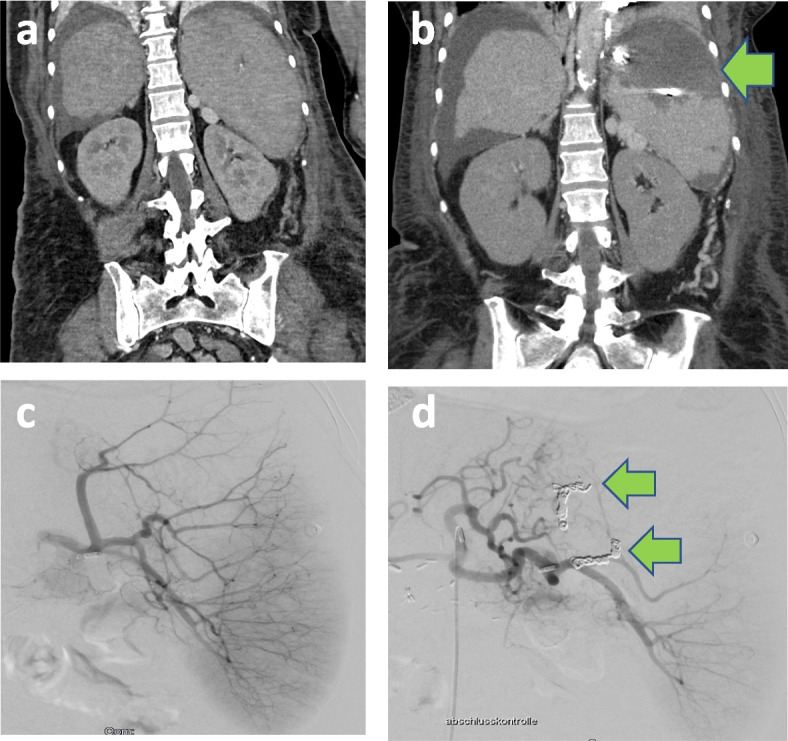
Background: Partial splenic embolization (PSE) is a non-surgical procedure which was initially used to treat hypersplenism. Furthermore, partial splenic embolization can be used for the treatment of different conditions, including gastroesophageal variceal hemorrhage. Here, we evaluated the safety and efficacy of emergency and non-emergency PSE in patients with gastroesophageal variceal hemorrhage and recurrent portal hypertensive gastropathy bleeding due to cirrhotic (CPH) and non-cirrhotic portal hypertension (NCPH).
Methods: From December 2014 to July 2022, twenty-five patients with persistent esophageal variceal hemorrhage (EVH) and gastric variceal hemorrhage (GVH), recurrent EVH and GVH, controlled EVH with a high risk of recurrent bleeding, controlled GVH with a high risk of rebleeding, and portal hypertensive gastropathy due to CPH and NCPH underwent emergency and non-emergency PSE. PSE for treatment of persistent EVH and GVH was defined as emergency PSE. In all patients pharmacological and endoscopic treatment alone had not been sufficient to control variceal bleeding, and the placement of a transjugular intrahepatic portosystemic shunt (TIPS) was contraindicated, not reasonable due to portal hemodynamics, or TIPS failure with recurrent esophageal bleeding had occurred. The patients were followed-up for six months.
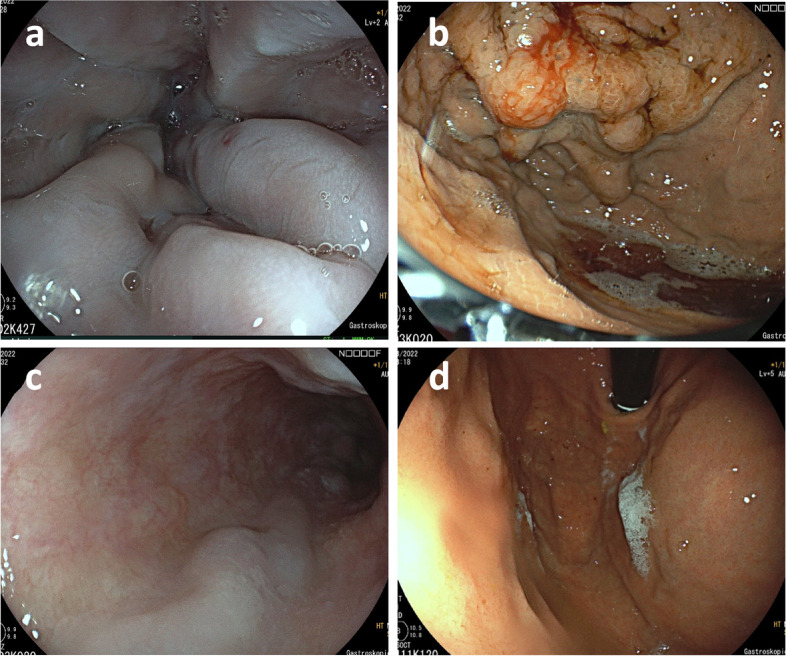
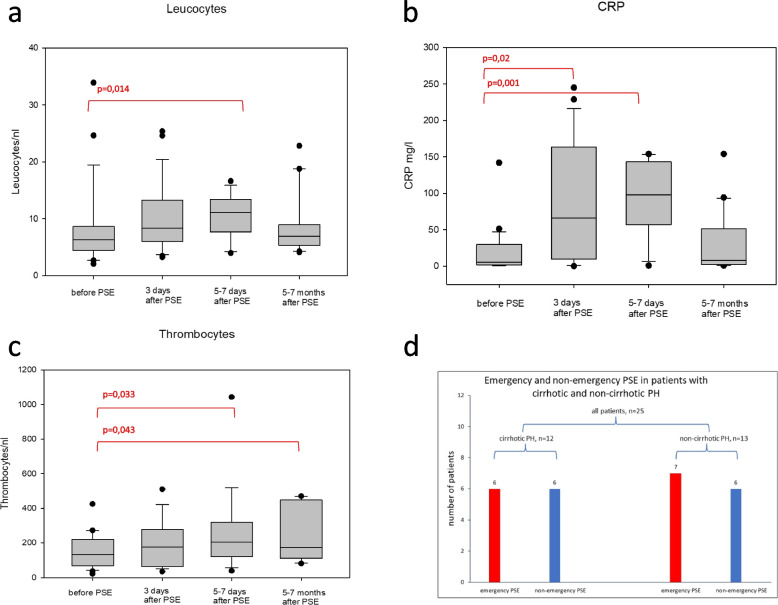
Results: All twenty-five patients, 12 with CPH and 13 with NCPH were successfully treated with PSE. In 13 out of 25 (52%) patients, PSE was performed under emergency conditions due to persistent EVH and GVH, clearly stopping the bleeding. Follow-up gastroscopy showed a significant regression of esophageal and gastric varices, classified as grade II or lower according to Paquet's classification after PSE in comparison to grade III to IV before PSE. During the follow-up period, no variceal re-bleeding occurred, neither in patients who were treated under emergency conditions nor in patients with non-emergency PSE. Furthermore, platelet count increased starting from day one after PSE, and after one week, thrombocyte levels had improved significantly. After six months, there was a sustained increase in the thrombocyte count at significantly higher levels. Fever, abdominal pain, and an increase in leucocyte count were transient side effects of the procedure. Severe complications were not observed.
Conclusion: This is the first study analyzing the efficacy of emergency and non-emergency PSE for the treatment of gastroesophageal hemorrhage and recurrent portal hypertensive gastropathy bleeding in patients with CPH and NCPH. We show that PSE is a successful rescue therapy for patients in whom pharmacological and endoscopic treatment options fail and the placement of a TIPS is contraindicated. In critically ill CPH and NCPH patients with fulminant gastroesophageal variceal bleeding, PSE showed good results and is therefore an effective tool for the rescue and emergency management of gastroesophageal hemorrhage.
Keywords: Acute-on-chronic liver failure; Cirrhotic portal hypertension; Esophageal varices; Gastric varices; Gastrointestinal hemorrhage; Liver cirrhosis; Non-cirrhotic portal hypertension; Partial splenic embolization; Portal hypertension.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of percutaneous transhepatic variceal embolization (PTVE) followed by partial splenic embolization versus PTVE alone for the treatment of acute esophagogastric variceal massive hemorrhage.J Vasc Interv Radiol. 2014 Dec;25(12):1858-65. doi: 10.1016/j.jvir.2014.08.019. Epub 2014 Oct 11. J Vasc Interv Radiol. 2014. PMID: 25311969
-
Portal vein thrombosis after partial splenic embolization in liver cirrhosis: efficacy of anticoagulation and long-term follow-up.J Vasc Interv Radiol. 2013 Dec;24(12):1808-16. doi: 10.1016/j.jvir.2013.08.018. Epub 2013 Oct 4. J Vasc Interv Radiol. 2013. PMID: 24099787
-
The Effect of Transjugular Intrahepatic Portosystemic Shunt Plus Partial Splenic Embolization for the Treatment of Patients with Recurrent Variceal Bleeding.Acad Radiol. 2020 Mar;27(3):323-331. doi: 10.1016/j.acra.2019.04.013. Epub 2019 May 28. Acad Radiol. 2020. PMID: 31147236
-
Transjugular Intrahepatic Portosystemic Shunt (TIPS): Pathophysiologic Basics, Actual Indications and Results with Review of the Literature.Rofo. 2018 Aug;190(8):701-711. doi: 10.1055/a-0628-7347. Epub 2018 Jul 25. Rofo. 2018. PMID: 30045395 Review. English, German.
-
Surgical portosystemic shunts versus transjugular intrahepatic portosystemic shunt for variceal haemorrhage in people with cirrhosis.Cochrane Database Syst Rev. 2018 Oct 31;10(10):CD001023. doi: 10.1002/14651858.CD001023.pub3. Cochrane Database Syst Rev. 2018. PMID: 30378107 Free PMC article.
Cited by
-
Splenic artery embolization for variceal bleeding in portal hypertension: a systematic review and metanalysis.Emerg Radiol. 2025 Feb;32(1):79-95. doi: 10.1007/s10140-024-02299-x. Epub 2024 Nov 22. Emerg Radiol. 2025. PMID: 39576386
-
Management Strategies for Refractory Esophageal Varices.DEN Open. 2025 Jun 19;6(1):e70155. doi: 10.1002/deo2.70155. eCollection 2026 Apr. DEN Open. 2025. PMID: 40538992 Free PMC article. Review.
-
Early Experience with Surgical Management of Non-Cirrhotic Portal Hypertension in Nigeria: Report from a Single Centre.J West Afr Coll Surg. 2025 Apr-Jun;15(2):176-180. doi: 10.4103/jwas.jwas_10_24. Epub 2024 Jul 18. J West Afr Coll Surg. 2025. PMID: 40094127 Free PMC article.
-
Chronic lymphocytic leukemia complicated by non-cirrhotic portal hypertension: an autopsy case report.Clin J Gastroenterol. 2025 Jul 16. doi: 10.1007/s12328-025-02184-1. Online ahead of print. Clin J Gastroenterol. 2025. PMID: 40668538
-
Partial splenectomy for massive malarial splenomegaly: A unique case from an Australian regional centre.Int J Surg Case Rep. 2025 Mar;128:111036. doi: 10.1016/j.ijscr.2025.111036. Epub 2025 Feb 7. Int J Surg Case Rep. 2025. PMID: 39956026 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
