

Large-vessel-occlusion in patients with previous ischemic stroke: an analysis of adherence to secondary preventive medication for different etiologies
- PMID: 37226225
- PMCID: PMC10210396
- DOI: 10.1186/s42466-023-00247-7
Large-vessel-occlusion in patients with previous ischemic stroke: an analysis of adherence to secondary preventive medication for different etiologies
Abstract
Background: Large vessel occlusion (LVO) is a severe condition that carries a high risk of morbidity and mortality, underscoring the importance of effective prevention strategies. This retrospective study aimed to analyze the intake of preventive medication at the time of hospitalization in a cohort of recurrent stroke patients presenting with acute LVO.
Methods: The study assessed the intake of either platelet aggregation inhibitors (PAI), oral anticoagulants (OAC) or statins at admission in patients with recurrent stroke and correlated it with the final classification of LVO. The frequency of those secondary preventive medication in recurrent stroke patients was defined as primary endpoint. The Modified Rankin Scale (mRS) at discharge was used as a functional outcome and defined as a secondary outcome measure.
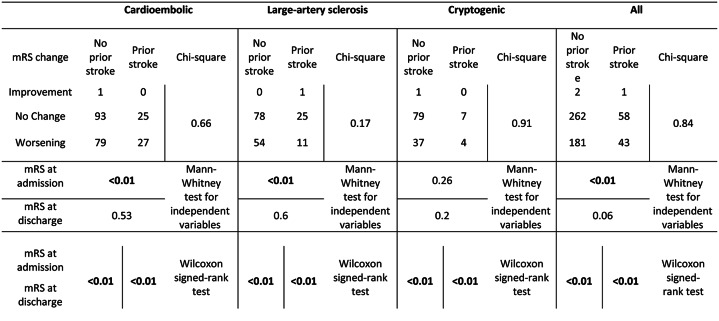
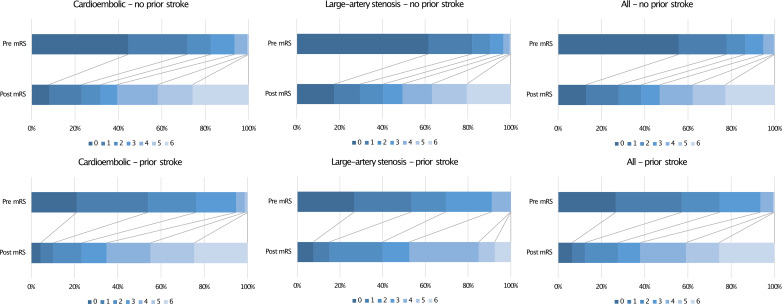
Results: This study included 866 patients who were treated for LVO between 2016 and 2020, of whom 160 (18.5%) had a recurrent ischemic stroke. OAC (25.6% vs. 14.1%, p < 0.01), PAI (50.0% vs. 26.0%, p < 0.01), or statin therapy (50.6% vs. 20.8%, p < 0.01) at admission were significantly more frequent in recurrent stroke patients compared to patients with a first-time stroke. Concerning LVO etiology in recurrent stroke patients, OAC at admission was taken in 46.8% of cardioembolic LVO, whereas PAI and statin at admission in macroangiopathic LVO were administered to 40.0%; neither PAI nor OAC was taken in 26.0%, 28.3%, and 31.6% of cardioembolic, macroangiopathic, or cryptogenic strokes, respectively. Regardless of stroke recurrence or etiology, there was an increase in mRS at discharge.
Conclusions: Despite high-quality healthcare, this study suggested a significant proportion of patients with recurrent stroke who were either non-adherent or insufficiently adherent to secondary preventive medication. Given the disability associated with LVO, improving patients' medication adherence and identifying unknown stroke causes are crucial for effective prevention strategies.
Keywords: Large vessel occlusion; Secondary prophylaxis; Stroke unit.
© 2023. The Author(s).
Conflict of interest statement
KK reports a grant from Merck Serono GmbH. FB reports personal fees and grants from AstraZeneca, Bristol-Myers Squibb (BMS), Boehringer, Laerdal and Stryker. FR reports personal fees from Angelini Pharma, Desitin Arzneimittel, Eisai GmbH, Jazz Pharma, Roche Pharma, UCB Pharma, and Zogenix and grants from the Detlev-Wrobel-Fonds for Epilepsy Research, the Chaja-Foundation Frankfurt, the Deutsche Forschungsgemeinschaft, the LOEWE Programme of the State of Hesse, and the European Union. FR reports, that he is a part of the editorial board of Neurological Research and Practice. AS reports personal fees and grants from Angelini Pharma/Arvelle Therapeutics, Desitin Arzneimittel, Eisai, Jazz (GW) Pharmaceuticals companies, Marinus Pharma, Takeda, UCB, UNEEG medical, and Zogenix. AS reports, that he is a part of the editorial board of Neurological Research and Practice. None of the other authors report conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources