

Robotic Versus Conventional or Endoscopic-assisted Nipple-sparing Mastectomy and Immediate Prosthesis Breast Reconstruction in the Management of Breast Cancer: A Prospectively Designed Multicenter Trial Comparing Clinical Outcomes, Medical Cost, and Patient-reported Outcomes (RCENSM-P)
- PMID: 37226826
- PMCID: PMC10727200
- DOI: 10.1097/SLA.0000000000005924
Robotic Versus Conventional or Endoscopic-assisted Nipple-sparing Mastectomy and Immediate Prosthesis Breast Reconstruction in the Management of Breast Cancer: A Prospectively Designed Multicenter Trial Comparing Clinical Outcomes, Medical Cost, and Patient-reported Outcomes (RCENSM-P)
Abstract
Objective: To compare the clinical and patient-reported outcomes of minimal access and conventional nipple-sparing mastectomy (C-NSM). The secondary outcomes investigated included medical costs and oncological safety.
Background: Minimal-access NSM has been increasingly applied in the treatment of patients with breast cancer. However, prospective multicenter trials comparing robotic-assisted NSM (R-NSM) versus C-NSM or endoscopic-assisted NSM (E-NSM) are lacking.
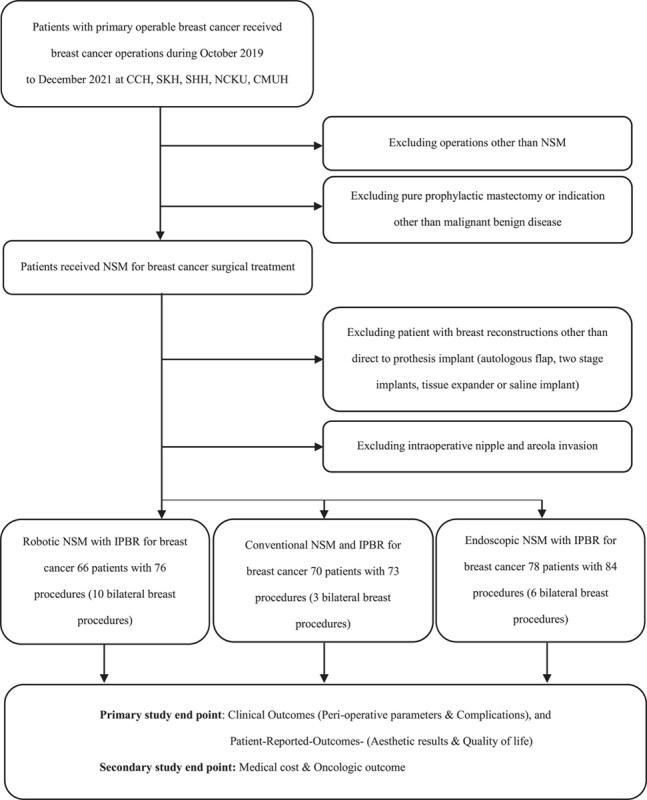
Methods: A prospectively designed 3-arm multicenter, nonrandomized trial (NCT04037852) was conducted from October 1, 2019 to December 31, 2021, to compare R-NSM with C-NSM or E-NSM.
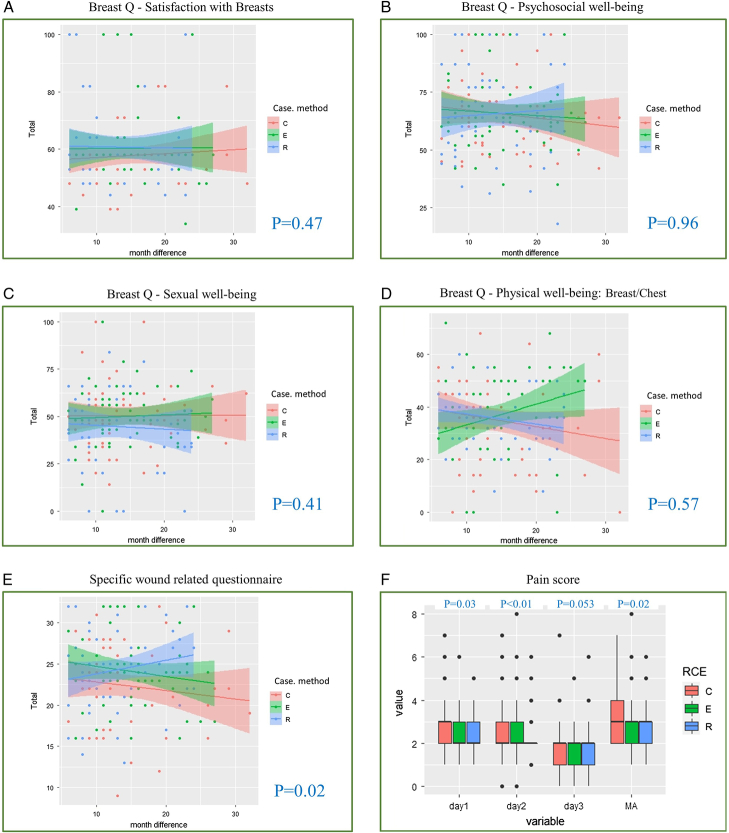
Results: A total of 73 R-NSM, 74 C-NSM, and 84 E-NSM procedures were enrolled. The median wound length and operation time of C-NSM was (9 cm, 175 minutes), (4 cm, and 195 minutes) in R-NSM, and (4 cm and 222 minutes) in E-NSM. Complications were comparable among the groups. Better wound healing was observed in the minimal-access NSM group. The R-NSM procedure was 4000 and 2600 United States Dollars more expensive than C-NSM and E-NSM, respectively. Wound/scar and postoperative acute pain evaluation favored the use of minimal access NSM over C-NSM. Quality of life in terms of chronic breast/chest pain, mobility, and range of motion of the upper extremity showed no significant differences. The preliminary oncologic results showed no differences among the 3 groups.
Conclusions: R-NSM or E-NSM is a safe alternative if compared with C-NSM in terms of perioperative morbidities, especially with better wound healing. The advantage of minimal access groups was higher wound-related satisfaction. Higher costs remain one of the major limiting factors in the widespread adoption of R-NSM.
Copyright © 2023 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Bailey CR, Ogbuagu O, Baltodano PA, et al. Quality-of-Life Outcomes Improve with Nipple-Sparing Mastectomy and Breast Reconstruction. Plast Reconstr Surg. 2017;140:219–226. - PubMed
-
- Cruz LDL, Moody AM, Tappy EE, et al. Overall survival, disease-free survival, local recurrence, and nipple-areolar recurrence in the setting of nipple-sparing mastectomy: a meta-analysis and systemic review. Ann Surg Oncol. 2015;22:3241–3249. - PubMed
-
- Lai HW, Lin SL, Chen ST, et al. Single-axillary-incision endoscopic-assisted hybrid technique for nipple-sparing mastectomy: technique, preliminary results, and patient-reported cosmetic outcome from preliminary 50 procedures. Ann Surg Oncol. 2018;25:1340–1349. - PubMed
-
- Lai HW, Chen ST, Mok CW, et al. Single-port three-dimensional (3D) videoscope-assisted endoscopic nipple-sparing mastectomy in the management of breast cancer: technique, clinical outcomes, medical cost, learning curve, and patient-reported aesthetic results from 80 preliminary procedures. Ann Surg Oncol. 2021;28:7331–7344. - PubMed
