

Multimodal hypersensitivity derived from quantitative sensory testing predicts pelvic pain outcome: an observational cohort study
- PMID: 37226937
- PMCID: PMC10440257
- DOI: 10.1097/j.pain.0000000000002909
Multimodal hypersensitivity derived from quantitative sensory testing predicts pelvic pain outcome: an observational cohort study
Abstract
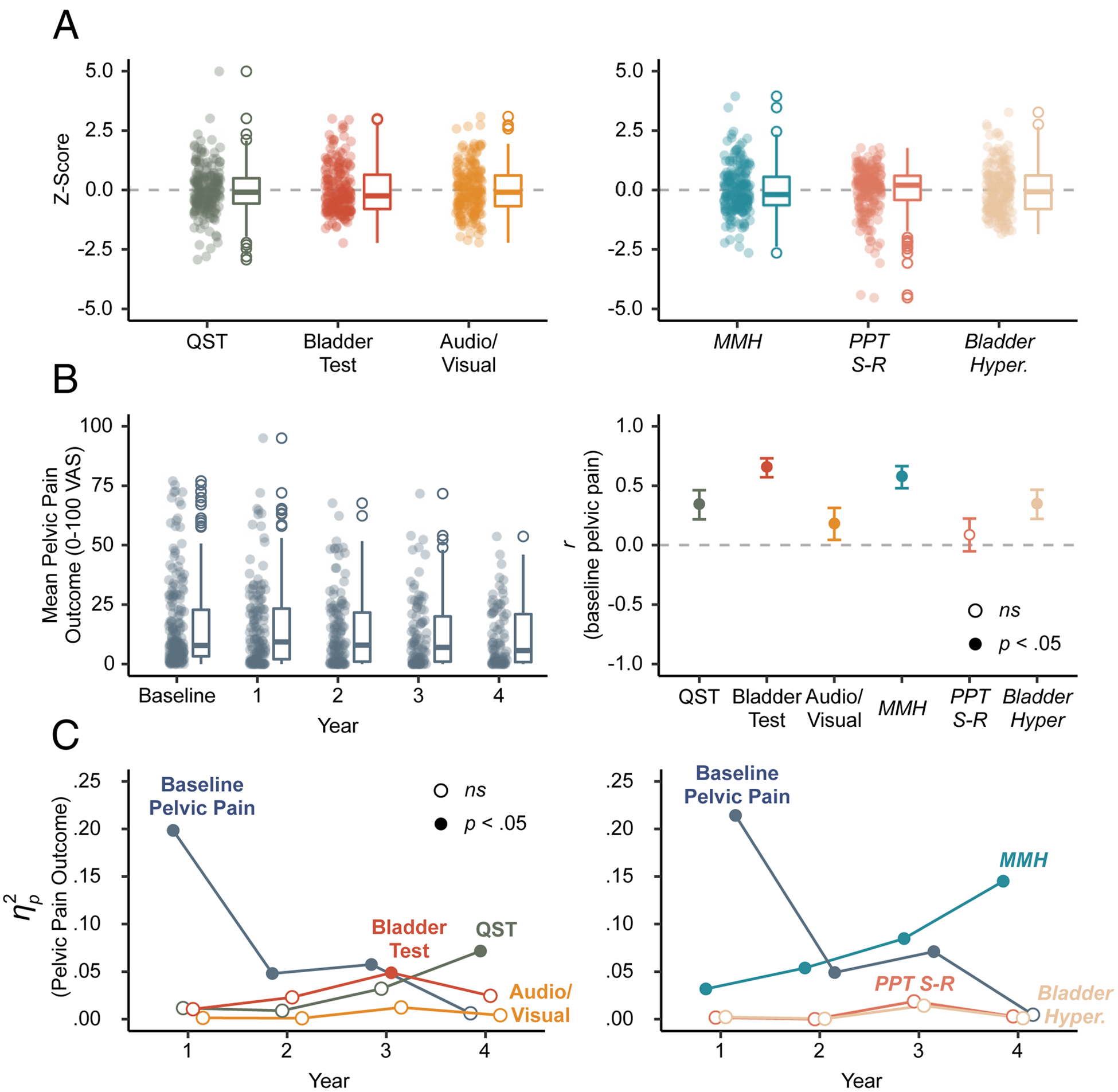
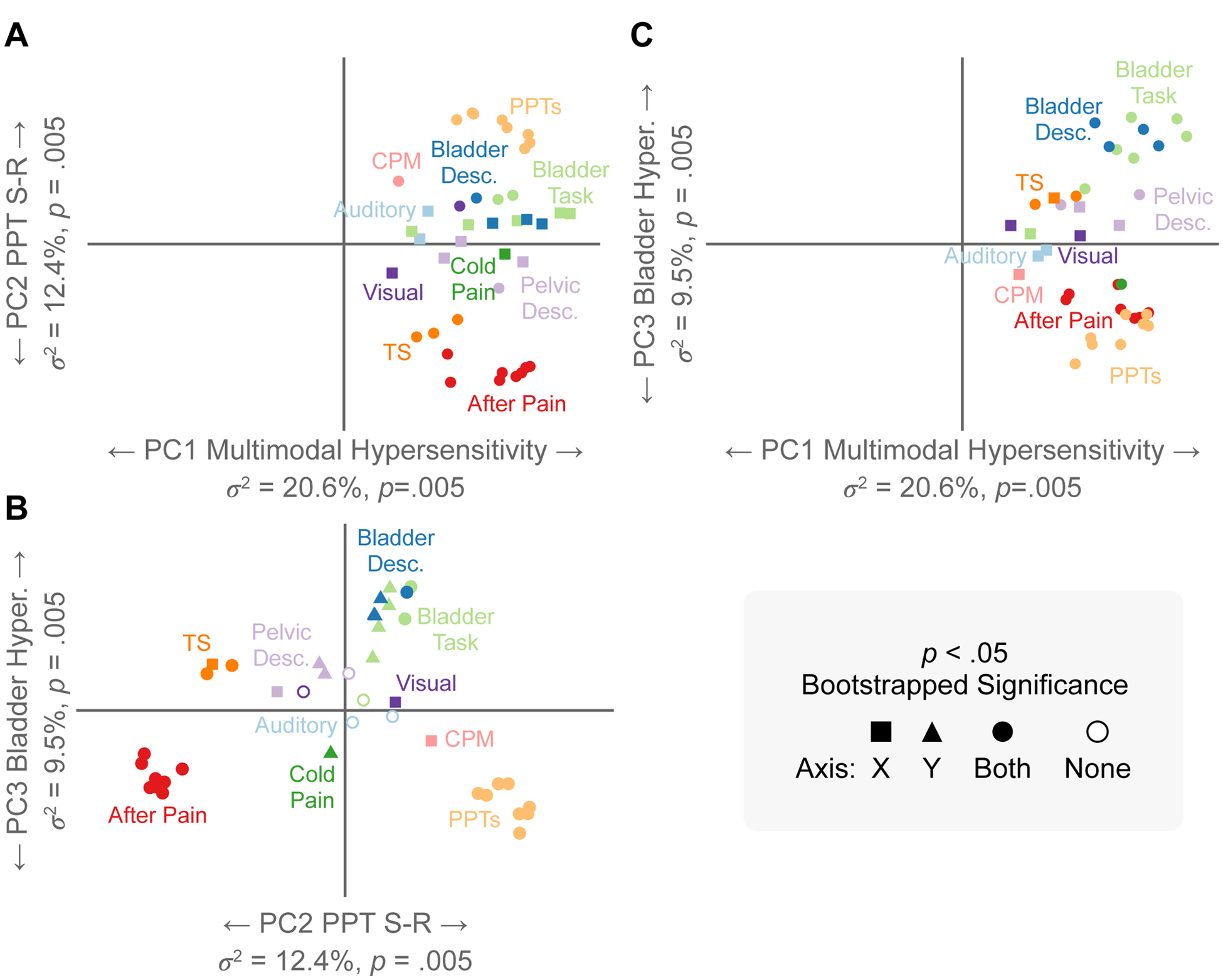
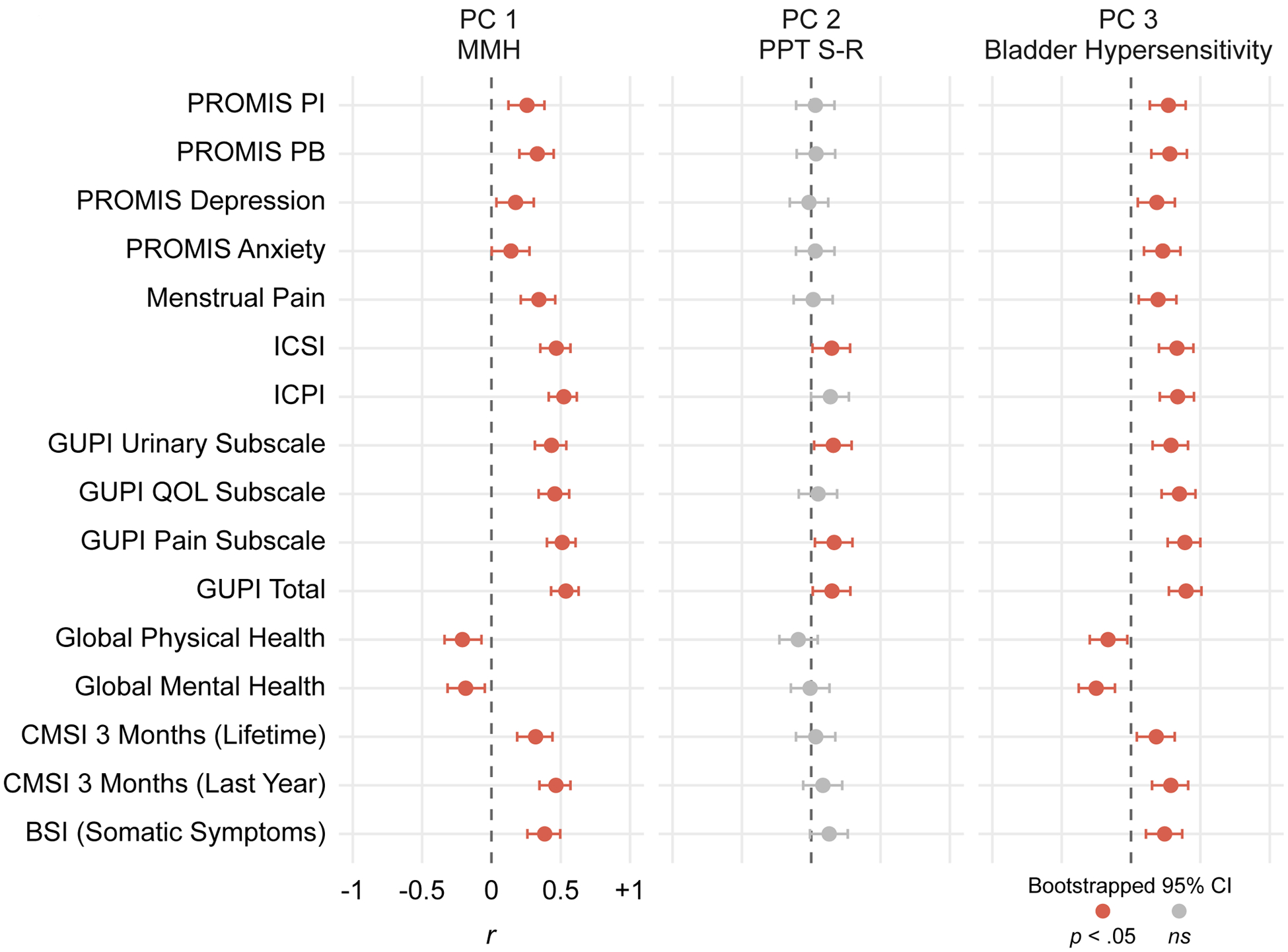
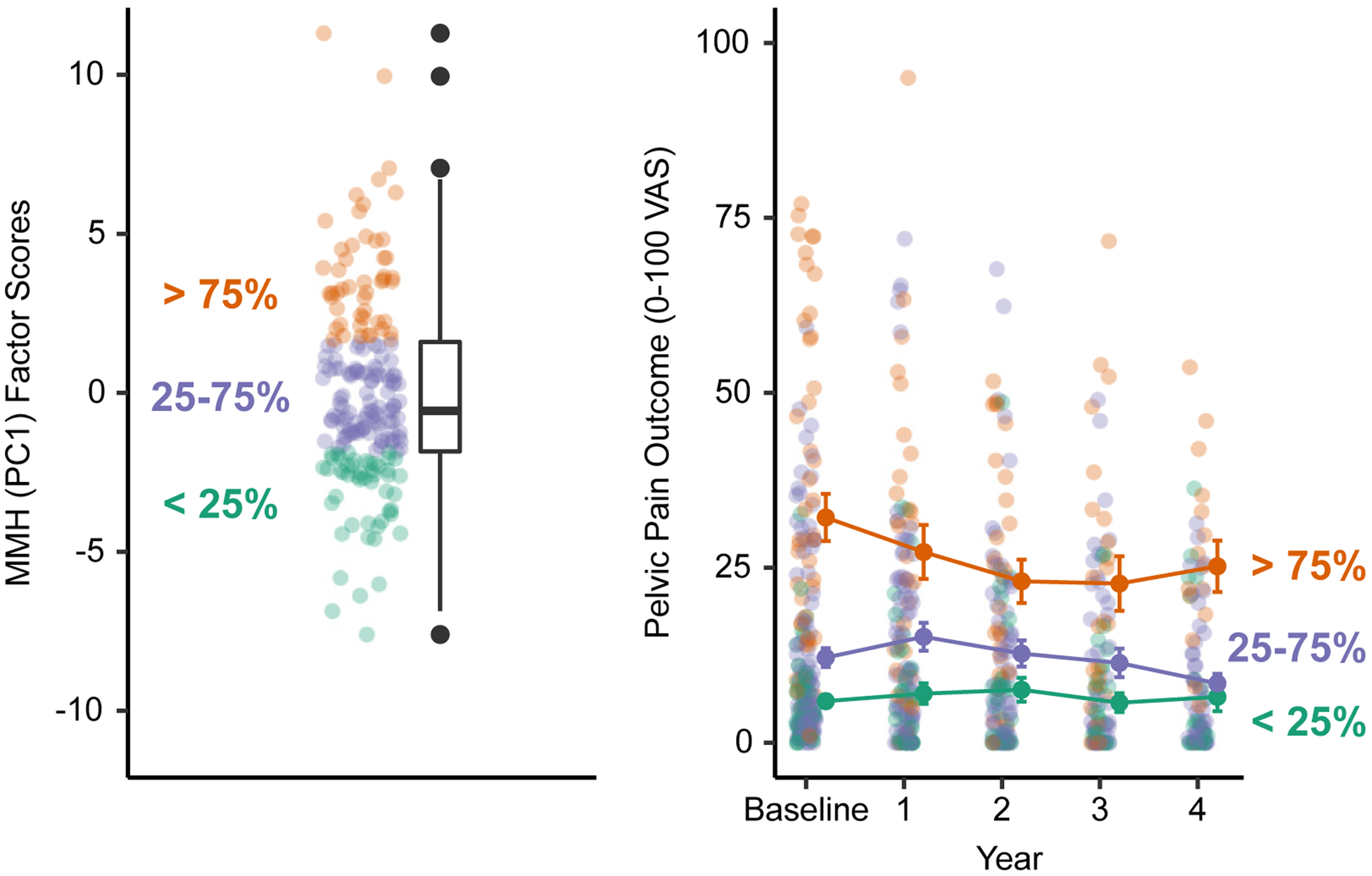
Multimodal hypersensitivity (MMH)-greater sensitivity across multiple sensory modalities (eg, light, sound, temperature, pressure)-is associated with the development of chronic pain. However, previous MMH studies are restricted given their reliance on self-reported questionnaires, narrow use of multimodal sensory testing, or limited follow-up. We conducted multimodal sensory testing on an observational cohort of 200 reproductive-aged women, including those at elevated risk for chronic pelvic pain conditions and pain-free controls. Multimodal sensory testing included visual, auditory, and bodily pressure, pelvic pressure, thermal, and bladder pain testing. Self-reported pelvic pain was examined over 4 years. A principal component analysis of sensory testing measures resulted in 3 orthogonal factors that explained 43% of the variance: MMH, pressure pain stimulus response, and bladder hypersensitivity. The MMH and bladder hypersensitivity factors correlated with baseline self-reported menstrual pain, genitourinary symptoms, depression, anxiety, and health. Over time, MMH increasingly predicted pelvic pain and was the only component to predict outcome 4 years later, even when adjusted for baseline pelvic pain. Multimodal hypersensitivity was a better predictor of pelvic pain outcome than a questionnaire-based assessment of generalized sensory sensitivity. These results suggest that MMHs overarching neural mechanisms convey more substantial long-term risk for pelvic pain than variation in individual sensory modalities. Further research on the modifiability of MMH could inform future treatment developments in chronic pain.
Trial registration: ClinicalTrials.gov NCT02214550.
Copyright © 2023 International Association for the Study of Pain.
Figures

References
-
- Abdi H Singular Value Decomposition (SVD) and Generalized Singular Value Decomposition (GSVD). Thousand Oaks, CA: Sage, 2007.
-
- Abdi H, Williams LJ. Principal component analysis. WIREs Comp Stat 2010;2:433–459.
-
- Andersson HI. The course of non-malignant chronic pain: a 12-year follow-up of a cohort from the general population. European Journal of Pain 2004;8:47–53. - PubMed
-
- Apkarian AV, Bushnell MC, Treede R-D, Zubieta J-K. Human brain mechanisms of pain perception and regulation in health and disease. European Journal of Pain 2005;9:463–463. - PubMed
-
- Arendt-Nielsen L Mechanistic similarities between fibromyalgia and other chronic pain conditions. PAIN Reports 2017;2:3.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
