

Determining resuscitation threshold for extremely preterm infants based on the survival rates without severe neurological injury
- PMID: 37227033
- PMCID: PMC10210526
- DOI: 10.7189/jogh.13.04059
Determining resuscitation threshold for extremely preterm infants based on the survival rates without severe neurological injury
Abstract
Background: Published guidelines on decision-making and resuscitation of extremely preterm infants primarily focus on high-income countries. For rapidly industrializing ones like China, there is a lack of population-based data for informing prenatal management and practice guidelines.
Methods: The Sino-northern Neonatal Network conducted a prospective multi-centre cohort study between 1 January 2018 and 31 December 2021. Infants with a gestational age (GA) between 22 (postnatal age in days = 0) and 28 (postnatal age in days = 6) admitted to 40 tertiary NICUs in northern China were included and evaluated for death or severe neurological injury before discharge.
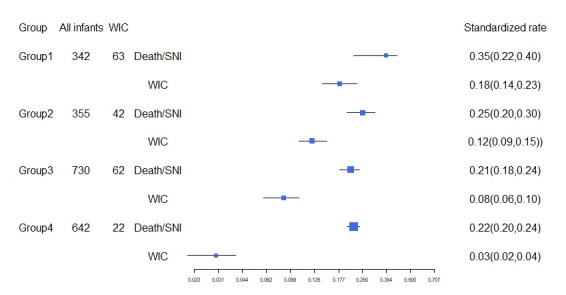
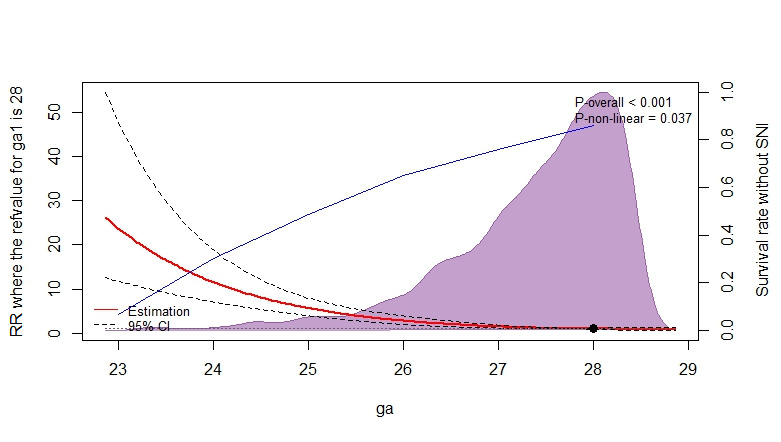
Results: For all extremely preterm infants (n = 5838), the proportion of admission to the neonatal was 4.1% at 22-24 weeks, 27.2% at 25-26 weeks, and 75.2% at 27 and 28 weeks. Among 2228 infants admitted to the NICU, 216 (11.1%) were still elected for withdrawal of care (WIC) due to non-medical factors. Survival rates without severe neurological injury were 6.7% for infants at 22-23 weeks, 28.0% at 24 weeks, 56.7% at 24 weeks, 61.7% at 25 weeks, 79.9% at 26 weeks, and 84.5% at 27 and 28 weeks. Compared with traditional criterion at 28 weeks, the relative risk for death or severe neurological injury were 1.53 (95% confidence interval (CI) = 1.26-1.86) at 27 weeks, 2.32 (95% CI = 1.73-3.11) at 26 weeks, 3.62 (95% CI = 2.43-5.40) at 25 weeks, and 8.91 (95% CI = 4.69-16.96) at 24 weeks. The NICUs with higher proportion of WIC also had a higher rate of death or severe neurological injury after maximal intensive care (MIC).
Conclusions: Compared to the traditional threshold of 28 weeks, more infants received MIC after 25 weeks, leading to significant increases in survival rates without severe neurological injury. Therefore, the resuscitation threshold should be gradually adjusted from 28 to 25 weeks based on reliable capacity.
Registration: China Clinical Trials Registry. ID: ChiCTR1900025234.
Copyright © 2023 by the Journal of Global Health. All rights reserved.
Conflict of interest statement
Disclosure of interest: The authors completed the ICMJE Disclosure of Interest Form (available upon request from the corresponding author) and disclose no relevant interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
