

Targeting the 16S rRNA Gene by Reverse Complement PCR Next-Generation Sequencing: Specific and Sensitive Detection and Identification of Microbes Directly in Clinical Samples
- PMID: 37227289
- PMCID: PMC10269728
- DOI: 10.1128/spectrum.04483-22
Targeting the 16S rRNA Gene by Reverse Complement PCR Next-Generation Sequencing: Specific and Sensitive Detection and Identification of Microbes Directly in Clinical Samples
Abstract
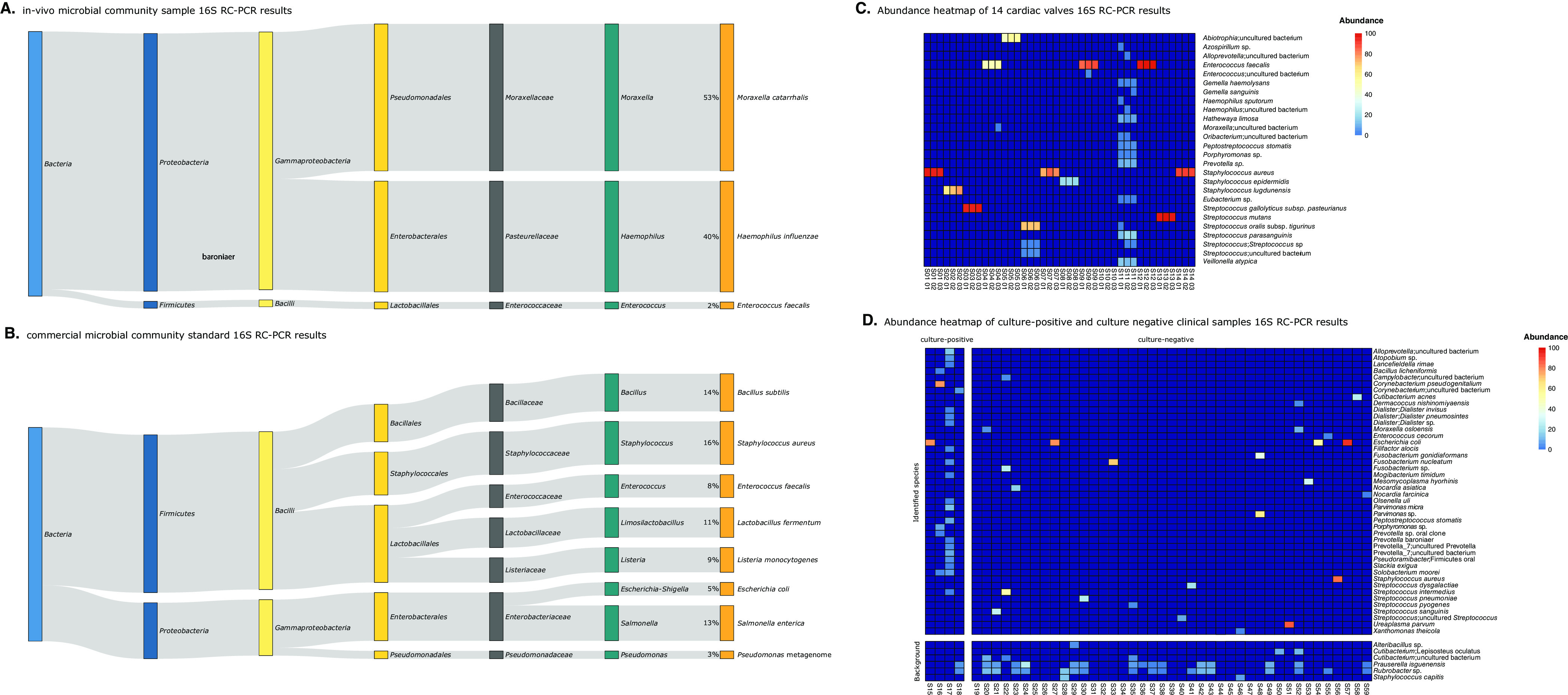
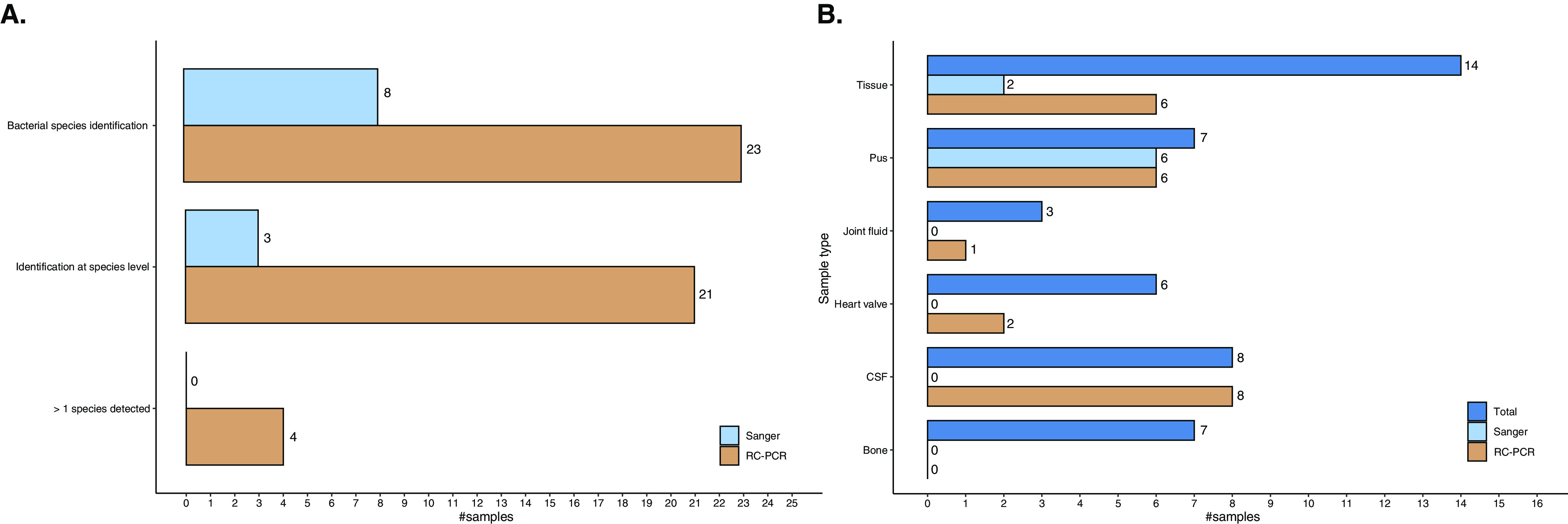
The detection and accurate identification of bacterial species in clinical samples are crucial for diagnosis and appropriate antibiotic treatment. To date, sequencing of the 16S rRNA gene has been widely used as a complementary molecular approach when identification by culture fails. The accuracy and sensitivity of this method are highly affected by the selection of the 16S rRNA gene region targeted. In this study, we assessed the clinical utility of 16S rRNA reverse complement PCR (16S RC-PCR), a novel method based on next-generation sequencing (NGS), for the identification of bacterial species. We investigated the performance of 16S RC-PCR on 11 bacterial isolates, 2 polymicrobial community samples, and 59 clinical samples from patients suspected of having a bacterial infection. The results were compared to culture results, if available, and to the results of Sanger sequencing of the 16S rRNA gene (16S Sanger sequencing). By 16S RC-PCR, all bacterial isolates were accurately identified to the species level. Furthermore, in culture-negative clinical samples, the rate of identification increased from 17.1% (7/41) to 46.3% (19/41) when comparing 16S Sanger sequencing to 16S RC-PCR. We conclude that the use of 16S RC-PCR in the clinical setting leads to an increased sensitivity of detection of bacterial pathogens, resulting in a higher number of diagnosed bacterial infections, and thereby can improve patient care. IMPORTANCE The identification of the causative infectious pathogen in patients suspected of having a bacterial infection is essential for diagnosis and the start of appropriate treatment. Over the past 2 decades, molecular diagnostics have improved the ability to detect and identify bacteria. However, novel techniques that can accurately detect and identify bacteria in clinical samples and that can be implemented in clinical diagnostics are needed. Here, we demonstrate the clinical utility of bacterial identification in clinical samples by a novel method called 16S RC-PCR. Using 16S RC-PCR, we reveal a significant increase in the number of clinical samples in which a potentially clinically relevant pathogen is identified compared to the commonly used 16S Sanger method. Moreover, RC-PCR allows automation and is well suited for implementation in a diagnostic laboratory. In conclusion, the implementation of this method as a diagnostic tool is expected to result in an increased number of diagnosed bacterial infections, and in combination with adequate treatment, this could improve clinical outcomes for patients.
Keywords: 16S rRNA; NGS; RC-PCR; bacterial identification; clinical diagnostics; infectious disease; molecular diagnostics; reverse complement PCR.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Johnson JS, Spakowicz DJ, Hong B-Y, Petersen LM, Demkowicz P, Chen L, Leopold SR, Hanson BM, Agresta HO, Gerstein M, Sodergren E, Weinstock GM. 2019. Evaluation of 16S rRNA gene sequencing for species and strain-level microbiome analysis. Nat Commun 10:5029. doi: 10.1038/s41467-019-13036-1. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
