

1-Year Incidence of Tuberculosis Infection and Disease Among Household Contacts of Rifampin- and Multidrug-Resistant Tuberculosis
- PMID: 37227925
- PMCID: PMC10681643
- DOI: 10.1093/cid/ciad301
1-Year Incidence of Tuberculosis Infection and Disease Among Household Contacts of Rifampin- and Multidrug-Resistant Tuberculosis
Abstract
Background: Tuberculosis infection (TBI) and TB disease (TBD) incidence remains poorly described following household contact (HHC) rifampin-/multidrug-resistant TB exposure. We sought to characterize TBI and TBD incidence at 1 year in HHCs and to evaluate TB preventive treatment (TPT) use in high-risk groups.
Methods: We previously conducted a cross-sectional study of HHCs with rifampin-/multidrug-resistant TB in 8 high-burden countries and reassessed TBI (interferon-gamma release assay, HHCs aged ≥5 years) and TBD (HHCs all ages) at 1 year. Incidence was estimated across age and risk groups (<5 years; ≥5 years, diagnosed with human immunodeficiency virus [HIV]; ≥5 years, not diagnosed with HIV/unknown, baseline TBI-positive) by logistic or log-binomial regression fitted using generalized estimating equations.
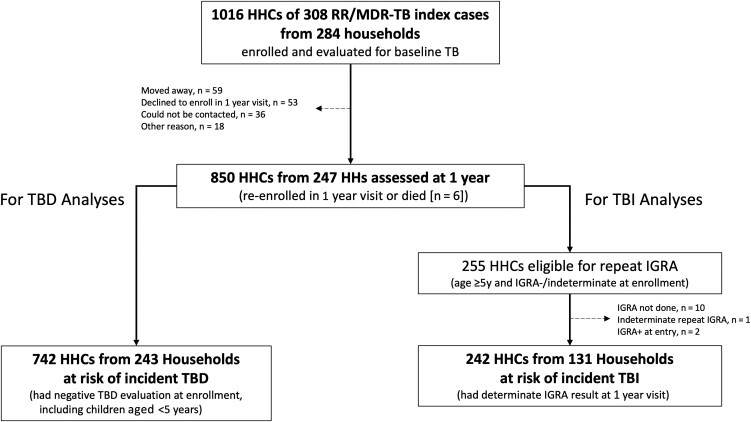
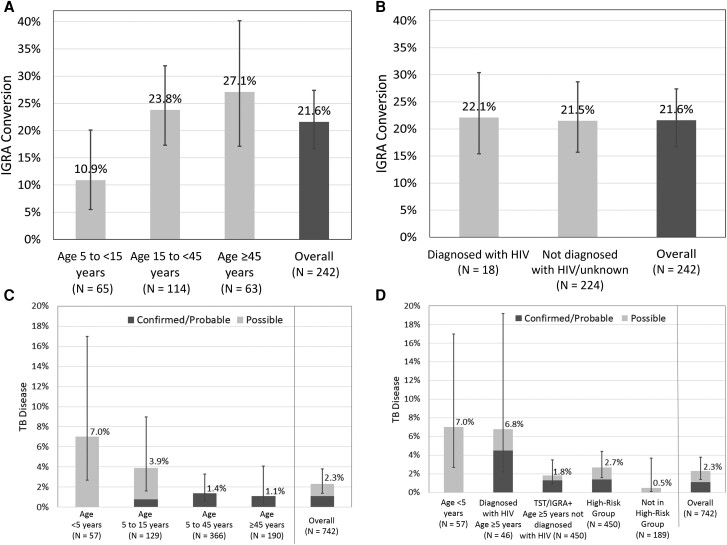
Results: Of 1016 HHCs, 850 (83.7%) from 247 households were assessed (median, 51.4 weeks). Among 242 HHCs, 52 tested interferon-gamma release assay-positive, yielding a 1-year 21.6% (95% confidence interval [CI], 16.7-27.4) TBI cumulative incidence. Sixteen of 742 HHCs developed confirmed (n = 5), probable (n = 3), or possible (n = 8) TBD, yielding a 2.3% (95% CI, 1.4-3.8) 1-year cumulative incidence (1.1%; 95% CI, .5-2.2 for confirmed/probable TBD). TBD relative risk was 11.5-fold (95% CI, 1.7-78.7), 10.4-fold (95% CI, 2.4-45.6), and 2.9-fold (95% CI, .5-17.8) higher in age <5 years, diagnosed with HIV, and baseline TBI high-risk groups, respectively, vs the not high-risk group (P = .0015). By 1 year, 4% (21 of 553) of high-risk HHCs had received TPT.
Conclusions: TBI and TBD incidence continued through 1 year in rifampin-/multidrug-resistant TB HHCs. Low TPT coverage emphasizes the need for evidence-based prevention and scale-up, particularly among high-risk groups.
Keywords: household contacts; multidrug-resistant tuberculosis; tuberculosis disease; tuberculosis infection; tuberculosis preventive treatment.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest . S. G. and V. M. report grant UM1AI069465 provided by NIAID. S. S. reports research grants from ViiV Healthcare (paid to institution) and unpaid participation as chair of an NIH, NIAID data and safety monitoring board (DSMB). S. Ki. reports grants from NIH (CRDF Global) and unpaid participation on the DRAMATIC Study DSMB. S. Kr. reports receipt of grants CRDF and RePORT India phase II, payment or honoraria from Clinical Care Options, LLC, and travel support from CROI 2022 New Investigator Scholarship. M. D. H. reports NIH research and training grants; travel support from CROI (paid to author); unpaid participation on a Medicins Sans Frontiers DSMB; and a role as board member for the Botswana Harvard Partnership via employer. A. G. reports grants or contracts from NIH, UNITAID, and the Centers for Disease Control and Prevention; travel support from CROI 2023 (paid to author); participation on the NIH/NAID Advisory Council and Indo US Science Technology Governing Board; and roles on the IMPAACT Network TB Scientific Committee and World Health Organization MDR TB Guidelines Committee. U. G. L. reports an ACTG NIH grant to a clinical research site. L. M. reports receipt of clinical trial fees to their institution from Merck Sharp & Dohme Corp, Adagio Therapeutics, Inc, ViiV Healthcare, and Johnson & Johnson. A. C. H. reports grant funding from DAIDS, NIAID, and NIH as one of the protocol chairs. G. C. reports a grant from DAID (paid to their institution). All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- World Health Organization . Global tuberculosis report 2022. Geneva, Switzerland: WHO, 2022. Available at: https://www.who.int/teams/global-tuberculosis-programme/tb-reports. Accessed 10 February 2023
-
- World Health Organization . Latent tuberculosis infection: updated and consolidated guidelines for programmatic management. Geneva, Switzerland: WHO, 2018. Report No.: 9789241550239. Available at: https://apps.who.int/iris/handle/10665/260233. Accessed 3 October 2022. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- UM1 AI069423/AI/NIAID NIH HHS/United States
- T32 AI007291/AI/NIAID NIH HHS/United States
- UM1 AI069456/AI/NIAID NIH HHS/United States
- HHSN275201800001C/HD/NICHD NIH HHS/United States
- UM1 AI068632/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- UM1 AI154463/AI/NIAID NIH HHS/United States
- K24 AI165099/AI/NIAID NIH HHS/United States
- P30 AI168386/AI/NIAID NIH HHS/United States
- UM1 AI106701/AI/NIAID NIH HHS/United States
- UM1 AI069465/AI/NIAID NIH HHS/United States
- UM1 AI106716/AI/NIAID NIH HHS/United States
- UM1 AI069463/AI/NIAID NIH HHS/United States
- UM1 AI068616/AI/NIAID NIH HHS/United States
- HHSN275201800001I/HD/NICHD NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
