

Dynamics of SARS-CoV-2 infection hospitalisation and infection fatality ratios over 23 months in England
- PMID: 37228015
- PMCID: PMC10212114
- DOI: 10.1371/journal.pbio.3002118
Dynamics of SARS-CoV-2 infection hospitalisation and infection fatality ratios over 23 months in England
Abstract
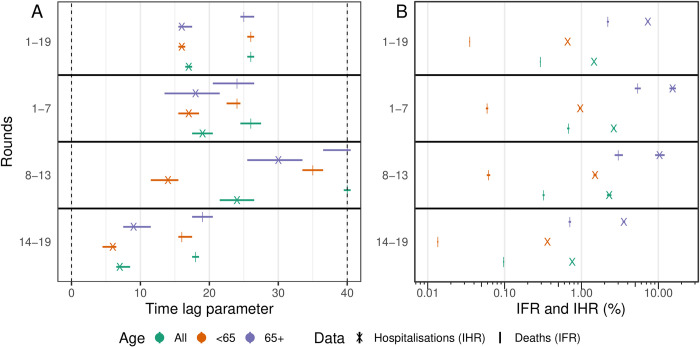
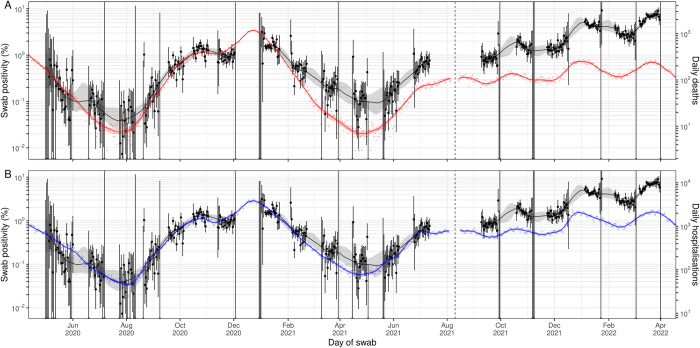
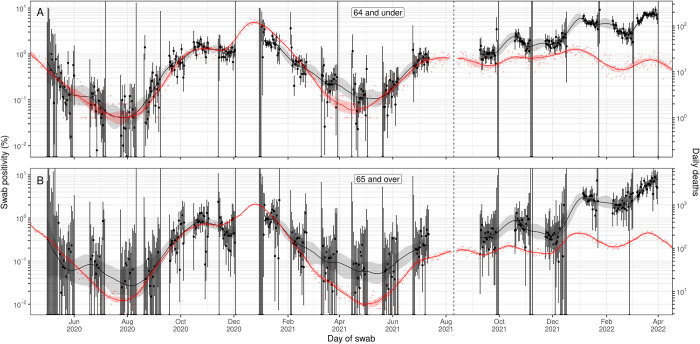
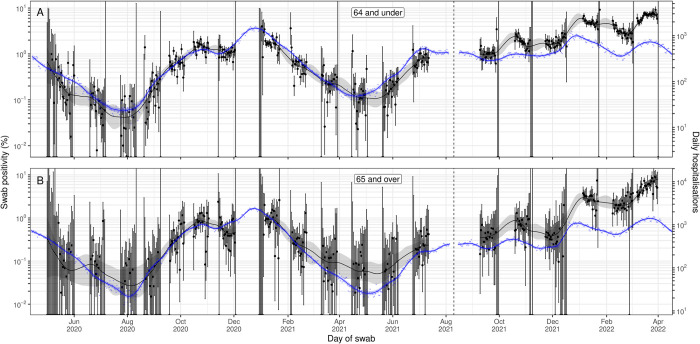
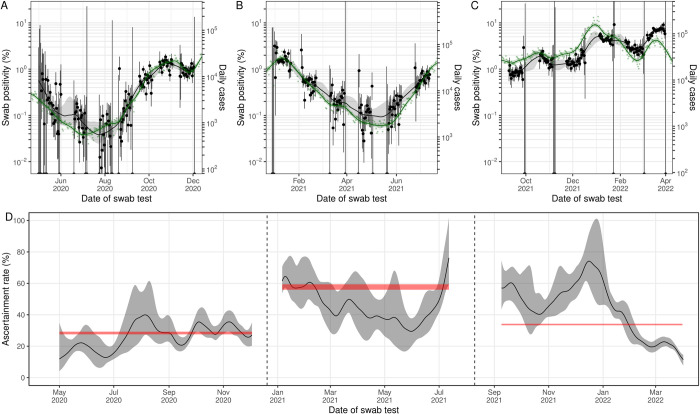
The relationship between prevalence of infection and severe outcomes such as hospitalisation and death changed over the course of the COVID-19 pandemic. Reliable estimates of the infection fatality ratio (IFR) and infection hospitalisation ratio (IHR) along with the time-delay between infection and hospitalisation/death can inform forecasts of the numbers/timing of severe outcomes and allow healthcare services to better prepare for periods of increased demand. The REal-time Assessment of Community Transmission-1 (REACT-1) study estimated swab positivity for Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection in England approximately monthly from May 2020 to March 2022. Here, we analyse the changing relationship between prevalence of swab positivity and the IFR and IHR over this period in England, using publicly available data for the daily number of deaths and hospitalisations, REACT-1 swab positivity data, time-delay models, and Bayesian P-spline models. We analyse data for all age groups together, as well as in 2 subgroups: those aged 65 and over and those aged 64 and under. Additionally, we analysed the relationship between swab positivity and daily case numbers to estimate the case ascertainment rate of England's mass testing programme. During 2020, we estimated the IFR to be 0.67% and the IHR to be 2.6%. By late 2021/early 2022, the IFR and IHR had both decreased to 0.097% and 0.76%, respectively. The average case ascertainment rate over the entire duration of the study was estimated to be 36.1%, but there was some significant variation in continuous estimates of the case ascertainment rate. Continuous estimates of the IFR and IHR of the virus were observed to increase during the periods of Alpha and Delta's emergence. During periods of vaccination rollout, and the emergence of the Omicron variant, the IFR and IHR decreased. During 2020, we estimated a time-lag of 19 days between hospitalisation and swab positivity, and 26 days between deaths and swab positivity. By late 2021/early 2022, these time-lags had decreased to 7 days for hospitalisations and 18 days for deaths. Even though many populations have high levels of immunity to SARS-CoV-2 from vaccination and natural infection, waning of immunity and variant emergence will continue to be an upwards pressure on the IHR and IFR. As investments in community surveillance of SARS-CoV-2 infection are scaled back, alternative methods are required to accurately track the ever-changing relationship between infection, hospitalisation, and death and hence provide vital information for healthcare provision and utilisation.
Copyright: © 2023 Eales et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Weekly epidemiological update on COVID-19 - 2021 May 11. [cited 2021 May 17]. Available from: https://www.who.int/publications/m/item/weekly-epidemiological-update-on...
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
