

Relationship of OCT-defined plaque characteristics with CCTA-derived coronary inflammation and CMR-derived global coronary flow reserve in patients with acute coronary syndrome
- PMID: 37228044
- PMCID: PMC10212089
- DOI: 10.1371/journal.pone.0286196
Relationship of OCT-defined plaque characteristics with CCTA-derived coronary inflammation and CMR-derived global coronary flow reserve in patients with acute coronary syndrome
Abstract
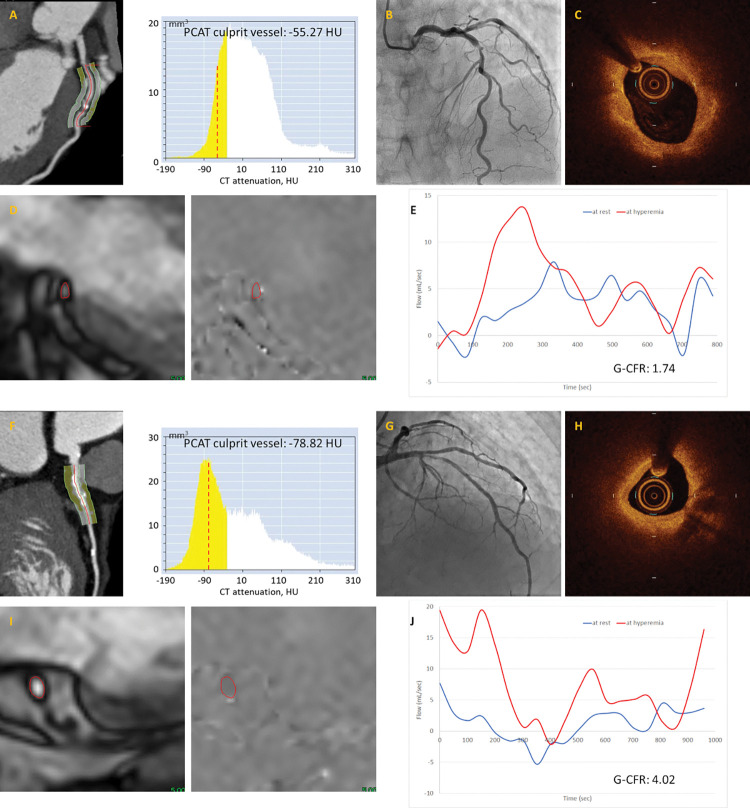
Background: The relationship of layered plaque detected by optical coherence tomography (OCT) with coronary inflammation and coronary flow reserve (CFR) remains elusive. We aimed to investigate the association of OCT-defined layered plaque with pericoronary adipose tissue (PCAT) inflammation assessed by coronary computed tomography angiography (CCTA) and global (G)-CFR assessed by cardiac magnetic resonance imaging (CMR) in patients with acute coronary syndrome (ACS).
Methods: We retrospectively investigated 88 patients with first ACS who underwent preprocedural CCTA, OCT imaging of the culprit lesion prior to primary/urgent percutaneous coronary intervention (PCI), and postprocedural CMR. All patients were divided into two groups according to the presence and absence of OCT-defined layered plaque at the culprit lesion. Coronary inflammation was assessed by the mean value of PCAT attenuation (-190 to -30 HU) of the three major coronary vessels. G-CFR was obtained by quantifying absolute coronary sinus flow at rest and during maximum hyperemia. CCTA and CMR findings were compared between the groups.
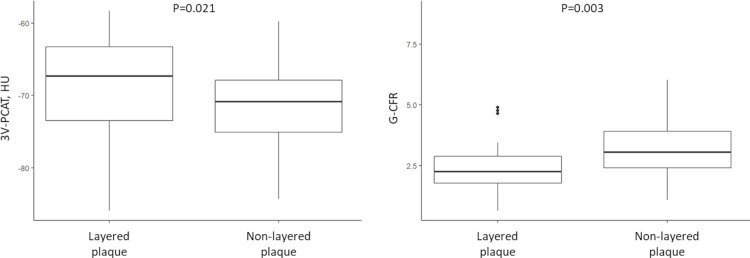
Results: In a total of 88 patients, layered plaque was detected in 51 patients (58.0%). The patients with layered plaque had higher three-vessel-PCAT attenuation value (-68.58 ± 6.41 vs. -71.60 ± 5.21 HU, P = 0.021) and culprit vessel-PCAT attenuation value (-67.69 ± 7.76 vs. -72.07 ± 6.57 HU, P = 0.007) than those with non-layered plaque. The patients with layered plaque had lower G-CFR value (median, 2.26 [interquartile range, 1.78, 2.89] vs. 3.06 [2.41, 3.90], P = 0.003) than those with non-layered plaque.
Conclusions: The presence of OCT-defined layered plaque at the culprit lesion was associated with high PCAT attenuation and low G-CFR after primary/urgent PCI in patients with ACS. OCT assessment of culprit plaque morphology and detection of layered plaque may help identify increased pericoronary inflammation and impaired CFR, potentially providing the risk stratification in patients with ACS and residual microvascular dysfunction after PCI.
Copyright: © 2023 Sugiyama et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Shimokado A, Matsuo Y, Kubo T, Nishiguchi T, Taruya A, Teraguchi I, et al. In vivo optical coherence tomography imaging and histopathology of healed coronary plaques. Atherosclerosis. 2018;275:35–42. - PubMed
-
- Oikonomou EK, Marwan M, Desai MY, Mancio J, Alashi A, Hutt Centeno E, et al. Non-invasive detection of coronary inflammation using computed tomography and prediction of residual cardiovascular risk (the CRISP CT study): a post-hoc analysis of prospective outcome data. Lancet. 2018;392(10151):929–39. doi: 10.1016/S0140-6736(18)31114-0 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
