

Effect of hip CPM on gross motor function and development of the hip joint: a single-center randomized controlled study on spastic cerebral palsy children with hip dysplasia
- PMID: 37228431
- PMCID: PMC10203473
- DOI: 10.3389/fped.2023.1090919
Effect of hip CPM on gross motor function and development of the hip joint: a single-center randomized controlled study on spastic cerebral palsy children with hip dysplasia
Abstract
Objective: To investigate the effectiveness of hip continuous passive motion (hCPM) on hip development at skeletal maturity and gross motor function for spastic cerebral palsy children with hip dysplasia.
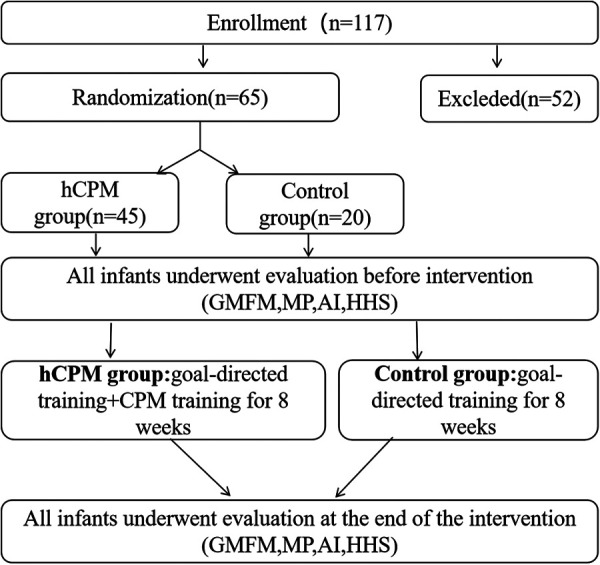
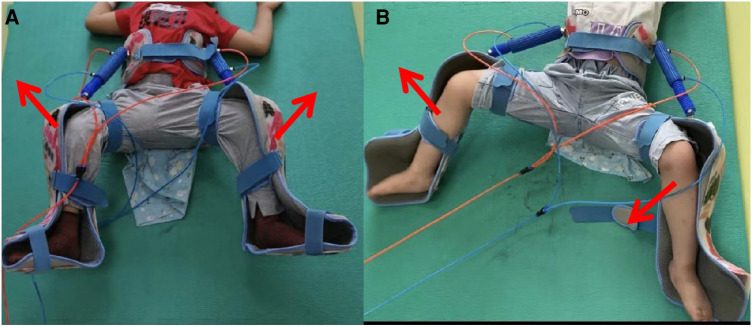
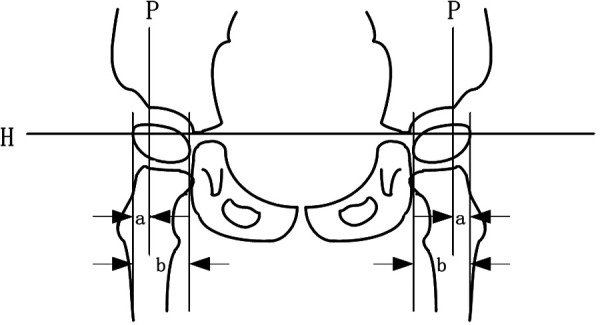
Methods: Prospective case-control research of hCPM with goal-directed training versus merely goal-directed training. On the basis of goal-directed training, the hCPM group used the hip joint CPM instrument (the external fixator was connected to the power device to make the hip joint carry out continuous passive movement) for 40-60 min, twice a day, and five times a week, and received continuous training for 8 weeks simultaneously. The control group received only goal-directed training for 8 weeks. Functional outcomes pertaining to the affected hip joints were assessed via gross motor function measure (GMFM), migration percentage (MP), acetabular index (AI), and Harris hip functional score (HHS) at the time of enrollment and the end of the intervention.
Results: The case-control research included 65 participants (mean age = 46.20 months, SD = 17.09 months; Gross Motor Function Grading System level: III = 41, IV = 24) who were randomly selected to either the hCPM (n = 45) or the control group (n = 20). No differences were found in baseline (acquisition phase) GMFM, MP, AI, or HHS (t = -1.720, P = 0.090; t* = 1.836, P* = 0.071; t# = -1.517, P# = 0.139; t* = -1.310, P* = 0.195; t# = -1.084, P# = 0.097; t = -1.041, P = 0.301). At the 8-week follow-up, GMFM, MP, AI, and HHS significantly improved over baseline in the hCPM group (hCPM group: t = 18.59, 20.172*, 40.291#, 16.820*, 32.900#, 28.081; P < 0.001). Between-group differences at 8-week follow-up times points favored the hCPM group for GMFM (t = -2.637, P = 0.011), MP (t* = 2.615, P* = 0.014; t# = 3.000, P# = 0.006), AI (t* = 2.055, P* = 0.044; t# = 2.223, P# = 0.030), HHS (t = -4.685, P < 0.001) (*: left side; #: right side).
Conclusion: Spastic cerebral palsy children with hip dysplasia achieved meaningful functional improvement after 8 weeks of goal-directed training with hCPM therapy.
Keywords: AI—acetabular index; GMFM—gross motor function measure; HHS—Harris hip functional score; MP—migration percentage; goal-directed; hCPM—hip continuous passive motion; hip continuous passive motion; hip dysplasia.
© 2023 Wang, Zhang, Fang, Cui, Niu, Lv, Hu and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources