

Ten-Year Multicenter Retrospective Study Utilizing Machine Learning Algorithms to Identify Patients at High Risk of Venous Thromboembolism After Radical Gastrectomy
- PMID: 37228741
- PMCID: PMC10202705
- DOI: 10.2147/IJGM.S408770
Ten-Year Multicenter Retrospective Study Utilizing Machine Learning Algorithms to Identify Patients at High Risk of Venous Thromboembolism After Radical Gastrectomy
Abstract
Purpose: This study aims to construct a machine learning model that can recognize preoperative, intraoperative, and postoperative high-risk indicators and predict the onset of venous thromboembolism (VTE) in patients.
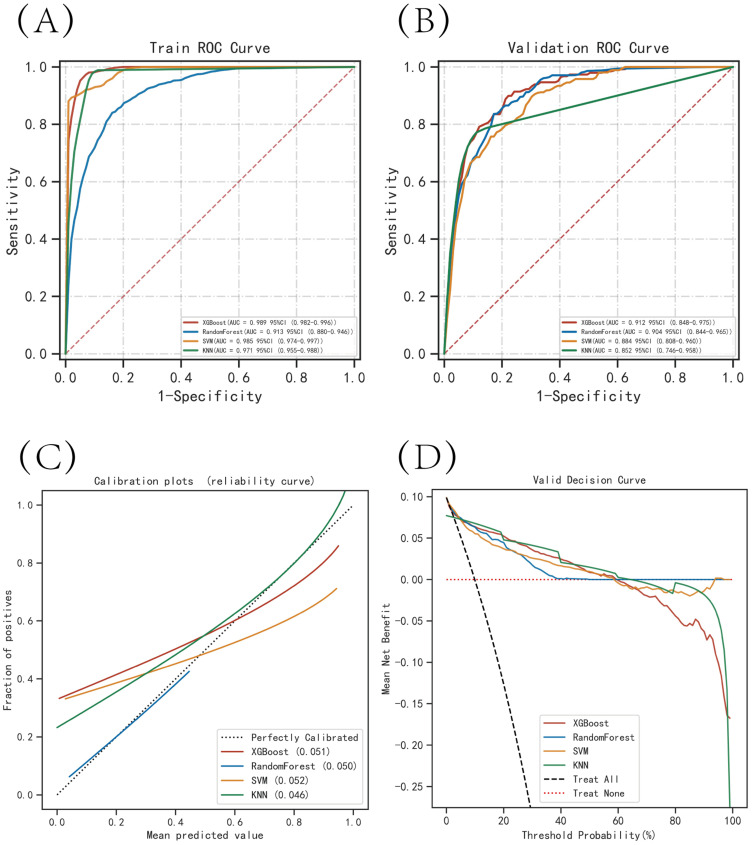
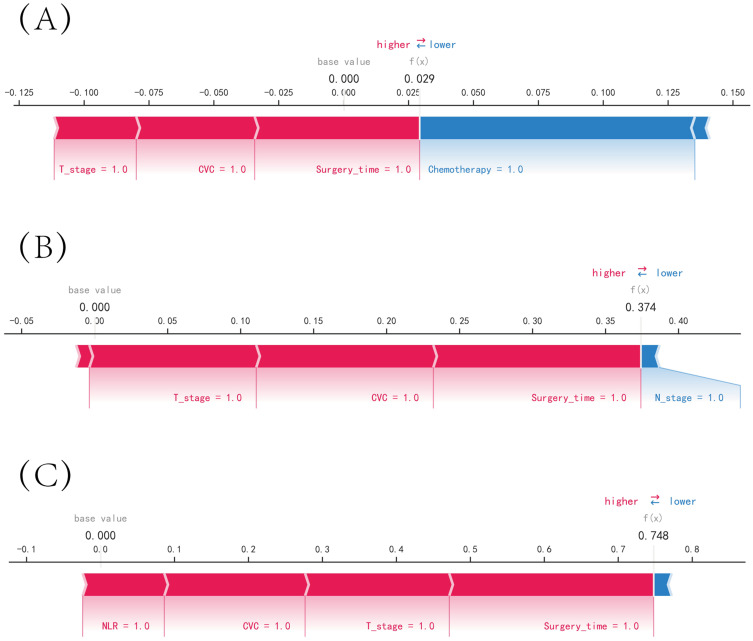
Patients and methods: A total of 1239 patients diagnosed with gastric cancer were enrolled in this retrospective study, among whom 107 patients developed VTE after surgery. We collected 42 characteristic variables of gastric cancer patients from the database of Wuxi People's Hospital and Wuxi Second People's Hospital between 2010 and 2020, including patients' demographic characteristics, chronic medical history, laboratory test characteristics, surgical information, and patients' postoperative conditions. Four machine learning algorithms, namely, extreme gradient boosting (XGBoost), random forest (RF), support vector machine (SVM), and k-nearest neighbor (KNN), were employed to develop predictive models. We also utilized Shapley additive explanation (SHAP) for model interpretation and evaluated the models using k-fold cross-validation, receiver operating characteristic (ROC) curves, calibration curves, decision curve analysis (DCA), and external validation metrics.
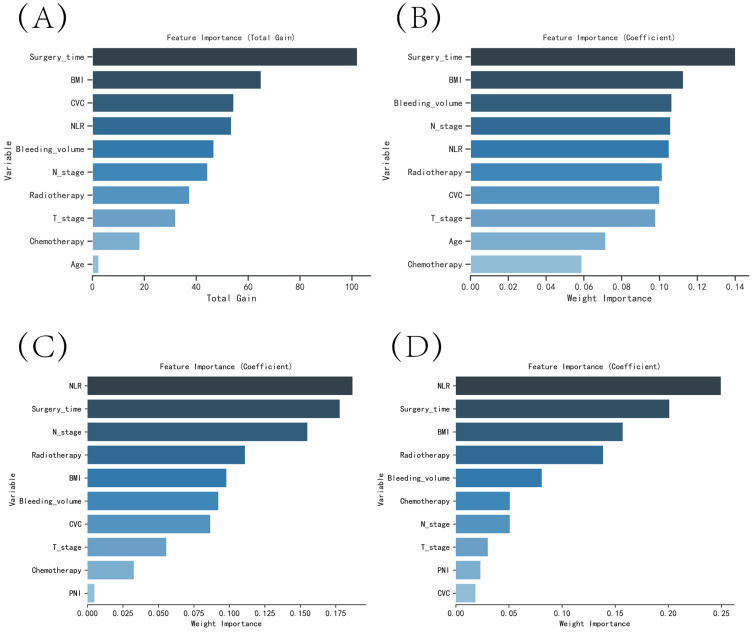
Results: The XGBoost algorithm demonstrated superior performance compared to the other three prediction models. The area under the curve (AUC) value for XGBoost was 0.989 in the training set and 0.912 in the validation set, indicating high prediction accuracy. Furthermore, the AUC value of the external validation set was 0.85, signifying good extrapolation of the XGBoost prediction model. The results of SHAP analysis revealed that several factors, including higher body mass index (BMI), history of adjuvant radiotherapy and chemotherapy, T-stage of the tumor, lymph node metastasis, central venous catheter use, high intraoperative bleeding, and long operative time, were significantly associated with postoperative VTE.
Conclusion: The machine learning algorithm XGBoost derived from this study enables the development of a predictive model for postoperative VTE in patients after radical gastrectomy, thereby assisting clinicians in making informed clinical decisions.
Keywords: gastrectomy; gastric neoplasms; machine learning; prediction model; risk factors; venous thromboembolism.
© 2023 Liu et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures



Similar articles
-
Using machine learning to identify patients at high risk of developing low bone density or osteoporosis after gastrectomy: a 10-year multicenter retrospective analysis.J Cancer Res Clin Oncol. 2023 Dec;149(19):17479-17493. doi: 10.1007/s00432-023-05472-w. Epub 2023 Oct 28. J Cancer Res Clin Oncol. 2023. PMID: 37897658 Free PMC article.
-
Utilizing machine learning algorithms for predicting risk factors for bone metastasis from right-sided colon carcinoma after complete mesocolic excision: a 10-year retrospective multicenter study.Discov Oncol. 2024 Sep 19;15(1):463. doi: 10.1007/s12672-024-01327-z. Discov Oncol. 2024. PMID: 39298052 Free PMC article.
-
Identification of High-Risk Patients for Postoperative Myocardial Injury After CME Using Machine Learning: A 10-Year Multicenter Retrospective Study.Int J Gen Med. 2023 Apr 7;16:1251-1264. doi: 10.2147/IJGM.S409363. eCollection 2023. Int J Gen Med. 2023. PMID: 37057054 Free PMC article.
-
Interpretable machine learning model to predict surgical difficulty in laparoscopic resection for rectal cancer.Front Oncol. 2024 Feb 6;14:1337219. doi: 10.3389/fonc.2024.1337219. eCollection 2024. Front Oncol. 2024. PMID: 38380369 Free PMC article. Review.
-
Risk factors of major bleeding detected by machine learning method in patients undergoing liver resection with controlled low central venous pressure technique.Postgrad Med J. 2023 Nov 20;99(1178):1280-1286. doi: 10.1093/postmj/qgad087. Postgrad Med J. 2023. PMID: 37794600 Review.
Cited by
-
Leveraging machine learning for enhanced and interpretable risk prediction of venous thromboembolism in acute ischemic stroke care.PLoS One. 2025 Mar 18;20(3):e0302676. doi: 10.1371/journal.pone.0302676. eCollection 2025. PLoS One. 2025. PMID: 40100876 Free PMC article.
-
Artificial intelligence in clinical thrombosis and hemostasis: A review.Res Pract Thromb Haemost. 2025 Jul 24;9(5):102984. doi: 10.1016/j.rpth.2025.102984. eCollection 2025 Jul. Res Pract Thromb Haemost. 2025. PMID: 40837028 Free PMC article. Review.
References
-
- Braumann C, Jacobi CA, Menenakos C, Ismail M, Rueckert JC, Mueller JM. Robotic-assisted laparoscopic and thoracoscopic surgery with the da Vinci system: a 4-year experience in a single institution. Surg Laparosc Endosc Percutan Tech. 2008;18(3):260–266. doi:10.1097/SLE.0b013e31816f85e5 - DOI - PubMed
LinkOut - more resources
Full Text Sources
