

Age‑adjusted Charlson comorbidity index and in‑hospital mortality in critically ill patients with cardiogenic shock: A retrospective cohort study
- PMID: 37229315
- PMCID: PMC10203756
- DOI: 10.3892/etm.2023.11998
Age‑adjusted Charlson comorbidity index and in‑hospital mortality in critically ill patients with cardiogenic shock: A retrospective cohort study
Abstract
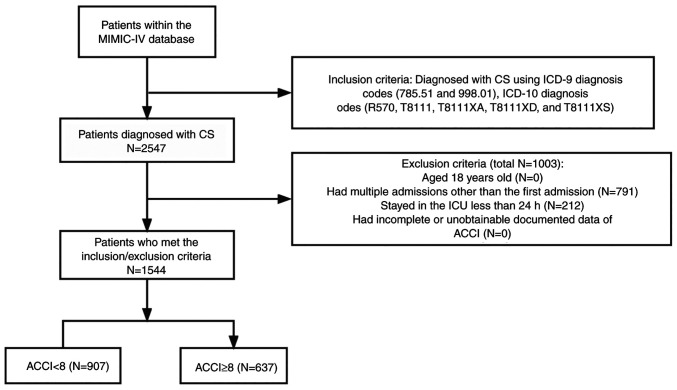
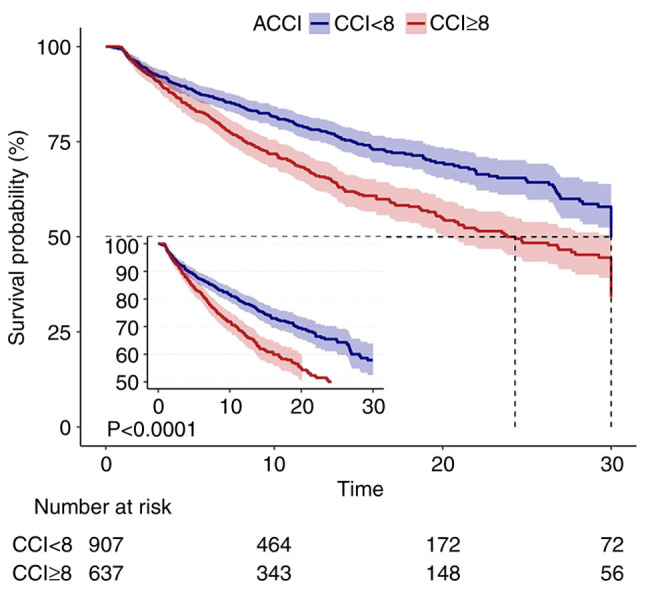
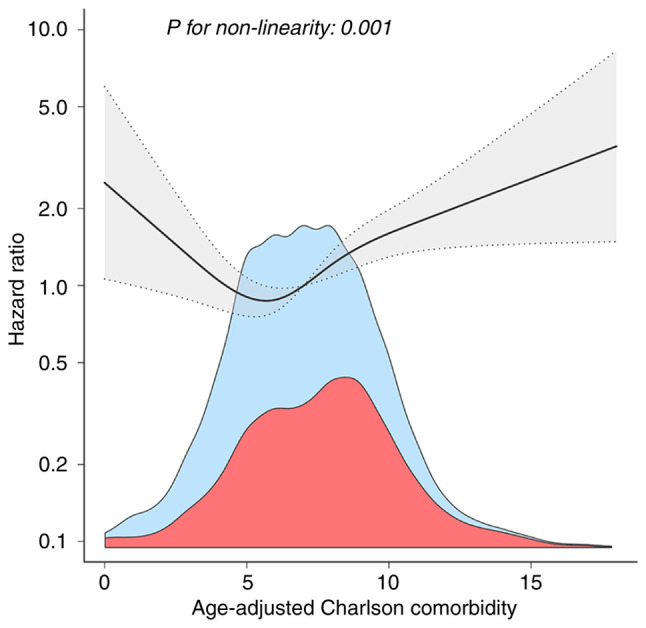
Evidence regarding the relationship between age-adjusted Charlson comorbidity index (ACCI) and in-hospital mortality is limited. Therefore, the present study investigated whether there was an independent association between ACCI and in-hospital mortality in critically ill patients with cardiogenic shock (CS) after adjusting for other covariates (age, sex, history of disease, scoring system, in-hospital management, vital signs at presentation, laboratory findings and vasopressors). ACCI, calculated retrospectively after hospitalization between 2008 and 2019, was derived from intensive care unit (ICU) admissions at the Beth Israel Deaconess Medical Center (Boston, MA, USA). Patients with CS were classified into two categories based on predefined ACCI scores (low, <8; high, ≥8). Based on baseline ACCI, the risk of in-hospital mortality in patients with CS was calculated using a multivariate Cox proportional risk model, and the threshold effect was calculated using a two-piece linear regression model. The in-hospital mortality rate was ~1.5 times greater in the ACCI high group compared with that in the ACCI low group [hazard ratio (HR)=1.45; 95% confidence interval (CI), 1.14-1.86]. Additional analysis showed that ACCI had a curvilinear association with in-hospital mortality risk in patients with CS, with a saturation effect predicted at 4.5. When ACCI was >4.5, the risk of in-hospital CS death increased significantly with increasing ACCI (HR=1.122; 95% CI, 1.054-1.194). Overall, ACCI was an independent predictor of in-hospital mortality in ICU patients with CS. A non-linear relationship was revealed between ACCI and in-hospital mortality, where in-hospital mortality increased significantly when ACCI was >4.5.
Keywords: age-adjusted Charlson comorbidity index; cardiogenic shock; intensive care unit; medical information mart for intensive care-IV; mortality.
Copyright: © Wei et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- van Diepen S, Katz JN, Albert NM, Henry TD, Jacobs AK, Kapur NK, Kilic A, Menon V, Ohman EM, Sweitzer NK, et al. Contemporary management of cardiogenic shock: A scientific statement from the American heart association. Circulation. 2017;136:e232–e268. doi: 10.1161/CIR.0000000000000525. - DOI - PubMed
-
- Goldberg RJ, Makam RCP, Yarzebski J, McManus DD, Lessard D, Gore JM. Decade-long trends (2001-2011) in the incidence and hospital death rates associated with the in-hospital development of cardiogenic shock after acute myocardial infarction. Circ Cardiovasc Qual Outcomes. 2016;9:117–125. doi: 10.1161/CIRCOUTCOMES.115.002359. - DOI - PMC - PubMed
-
- Alizadeh AM, Hassanian-Moghaddam H, Shadnia S, Zamani N, Mehrpour O. Simplified acute physiology score II/acute physiology and chronic health evaluation II and prediction of the mortality and later development of complications in poisoned patients admitted to intensive care unit. Basic Clin Pharmacol Toxicol. 2014;115:297–300. doi: 10.1111/bcpt.12210. - DOI - PubMed
LinkOut - more resources
Full Text Sources