

Global disparities in mortality and liver transplantation in hospitalised patients with cirrhosis: a prospective cohort study for the CLEARED Consortium
- PMID: 37230109
- PMCID: PMC10330833
- DOI: 10.1016/S2468-1253(23)00098-5
Global disparities in mortality and liver transplantation in hospitalised patients with cirrhosis: a prospective cohort study for the CLEARED Consortium
Abstract
Background: Cirrhosis, the end result of liver injury, has high mortality globally. The effect of country-level income on mortality from cirrhosis is unclear. We aimed to assess predictors of death in inpatients with cirrhosis using a global consortium focusing on cirrhosis-related and access-related variables.
Methods: In this prospective observational cohort study, the CLEARED Consortium followed up inpatients with cirrhosis at 90 tertiary care hospitals in 25 countries across six continents. Consecutive patients older than 18 years who were admitted non-electively, without COVID-19 or advanced hepatocellular carcinoma, were enrolled. We ensured equitable participation by limiting enrolment to a maximum of 50 patients per site. Data were collected from patients and their medical records, and included demographic characteristics; country; disease severity (MELD-Na score); cirrhosis cause; medications used; reasons for admission; transplantation listing; cirrhosis-related history in the past 6 months; and clinical course and management while hospitalised and for 30 days post discharge. Primary outcomes were death and receipt of liver transplant during index hospitalisation or within 30 days post discharge. Sites were surveyed regarding availability of and access to diagnostic and treatment services. Outcomes were compared by country income level of participating sites, defined according to World Bank income classifications (high-income countries [HICs], upper-middle-income countries [UMICs], and low-income or lower-middle-income countries [LICs or LMICs]). Multivariable models controlling for demographic variables, disease cause, and disease severity were used to analyse the odds of each outcome associated with variables of interest.
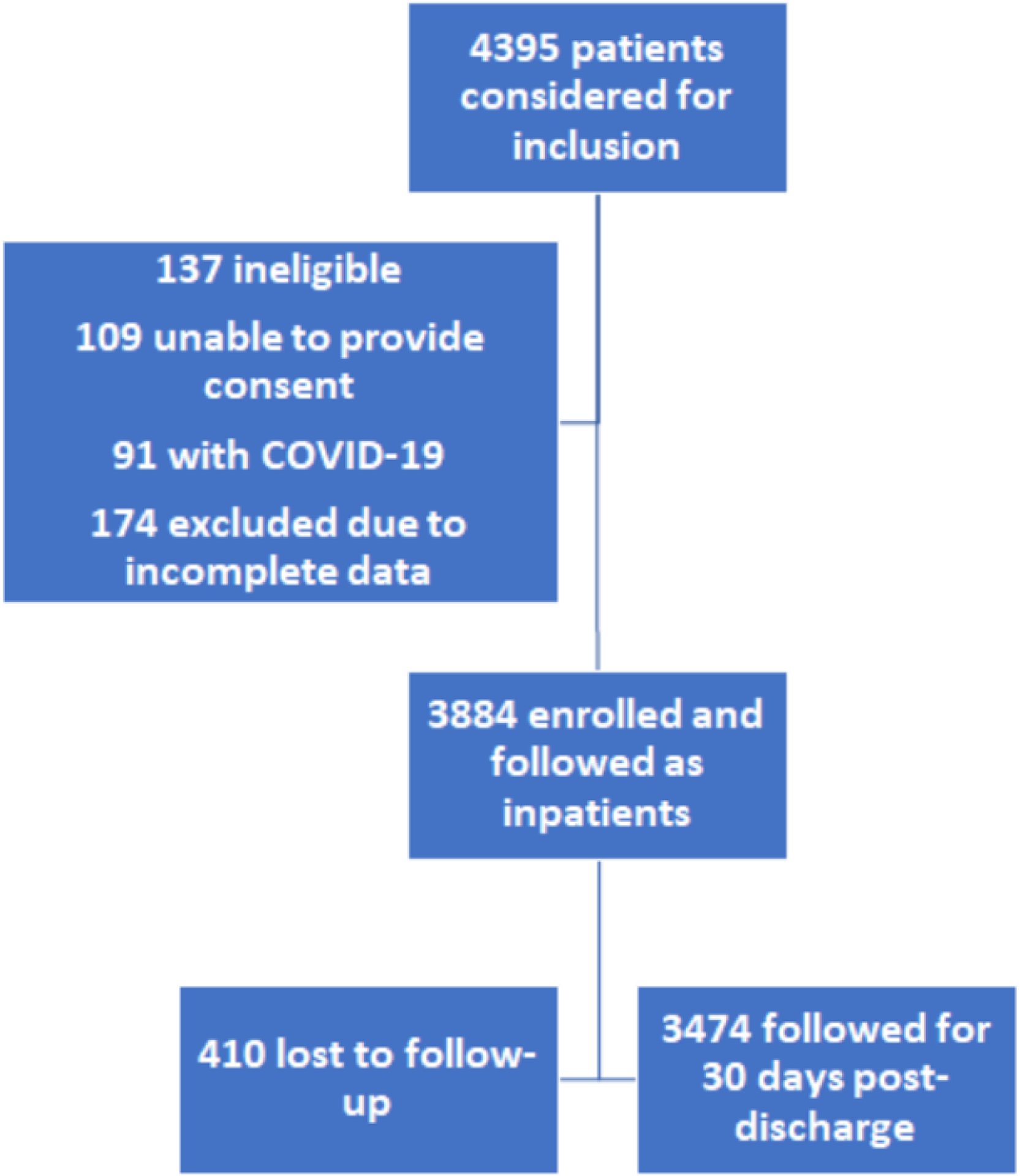
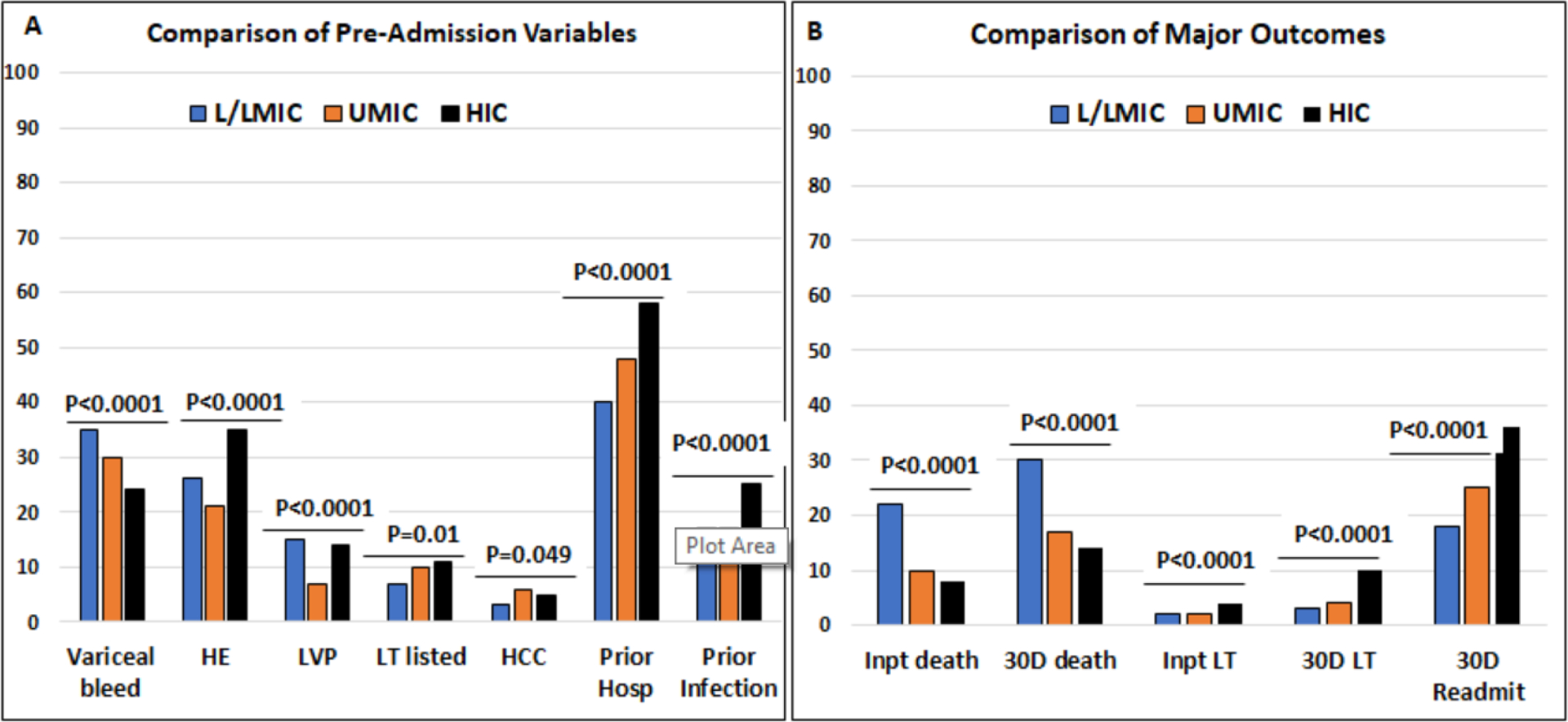
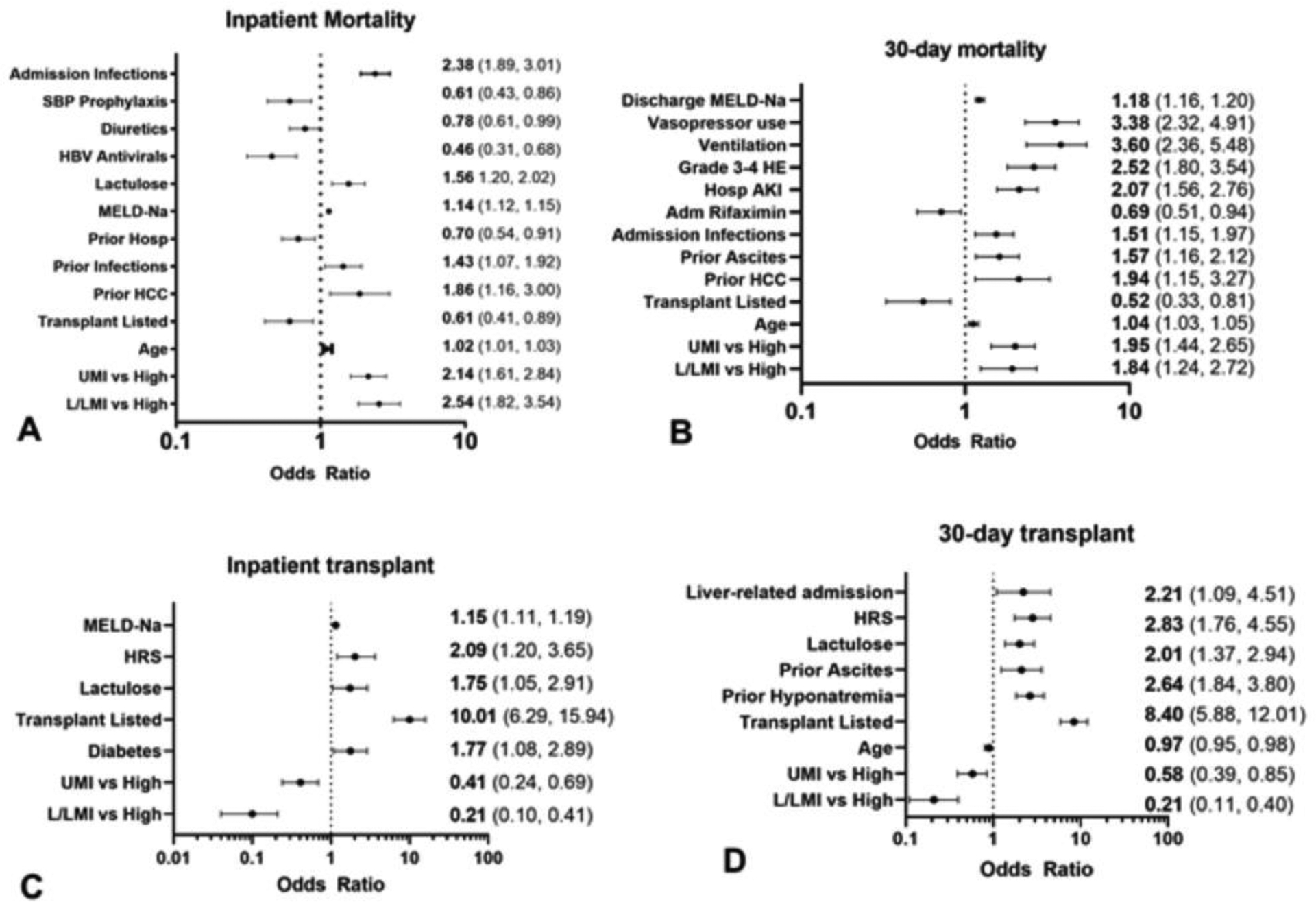
Findings: Patients were recruited between Nov 5, 2021, and Aug 31, 2022. Complete inpatient data were obtained for 3884 patients (mean age 55·9 years [SD 13·3]; 2493 (64·2%) men and 1391 (35·8%) women; 1413 [36·4%] from HICs, 1757 [45·2%] from UMICs, and 714 [18·4%] from LICs or LMICs), with 410 lost to follow-up within 30 days after hospital discharge. The number of patients who died while hospitalised was 110 (7·8%) of 1413 in HICs, 182 (10·4%) of 1757 in UMICs, and 158 (22·1%) of 714 in LICs and LMICs (p<0·0001), and within 30 days post discharge these values were 179 (14·4%) of 1244 in HICs, 267 (17·2%) of 1556 in UMICs, and 204 (30·3%) of 674 in LICs and LMICs (p<0·0001). Compared with patients from HICs, increased risk of death during hospitalisation was found for patients from UMICs (adjusted odds ratio [aOR] 2·14 [95% CI 1·61-2·84]) and from LICs or LMICs (2·54 [1·82-3·54]), in addition to increased risk of death within 30 days post discharge (1·95 [1·44-2·65] in UMICs and 1·84 [1·24-2·72] in LICs or LMICs). Receipt of a liver transplant was recorded in 59 (4·2%) of 1413 patients from HICs, 28 (1·6%) of 1757 from UMICs (aOR 0·41 [95% CI 0·24-0·69] vs HICs), and 14 (2·0%) of 714 from LICs and LMICs (0·21 [0·10-0·41] vs HICs) during index hospitalisation (p<0·0001), and in 105 (9·2%) of 1137 patients from HICs, 55 (4·0%) of 1372 from UMICs (0·58 [0·39-0·85] vs HICs), and 16 (3·1%) of 509 from LICs or LMICs (0·21 [0·11-0·40] vs HICs) by 30 days post discharge (p<0·0001). Site survey results showed that access to important medications (rifaximin, albumin, and terlipressin) and interventions (emergency endoscopy, liver transplantation, intensive care, and palliative care) varied geographically.
Interpretation: Inpatients with cirrhosis in LICs, LMICs, or UMICs have significantly higher mortality than inpatients in HICs independent of medical risk factors, and this might be due to disparities in access to essential diagnostic and treatment services. These results should encourage researchers and policy makers to consider access to services and medications when evaluating cirrhosis-related outcomes.
Funding: National Institutes of Health and US Department of Veterans Affairs.
Copyright © 2023 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests JSB has received grants to his institution from the NIH and is editor-in-chief and board of trustees member for the American College of Gastroenterology. All other authors declare no competing interests.
Figures
References
-
- Asrani SK, Devarbhavi H, Eaton J, Kamath PS. Burden of liver diseases in the world. J Hepatol 2019; 70(1): 151–71. - PubMed
-
- Vento S, Cainelli F. Chronic liver diseases must be reduced worldwide: it is time to act. Lancet Glob Health 2022; 10(4): e471–e2. - PubMed
-
- Bajaj JS, Kamath PS, Reddy KR. The Evolving Challenge of Infections in Cirrhosis. N Engl J Med 2021; 384(24): 2317–30. - PubMed
-
- Ma C, Qian AS, Nguyen NH, et al. Trends in the Economic Burden of Chronic Liver Diseases and Cirrhosis in the United States: 1996–2016. Am J Gastroenterol 2021; 116(10): 2060–7. - PubMed
-
- O’Leary JG, Reddy KR, Garcia-Tsao G, et al. NACSELD Acute-on-Chronic Liver Failure (NACSELD-ACLF) Score Predicts 30-Day Survival in Hospitalized Patients with Cirrhosis. Hepatology 2018. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
