

Normothermic machine perfusion versus static cold storage in donation after circulatory death kidney transplantation: a randomized controlled trial
- PMID: 37231075
- PMCID: PMC10287561
- DOI: 10.1038/s41591-023-02376-7
Normothermic machine perfusion versus static cold storage in donation after circulatory death kidney transplantation: a randomized controlled trial
Abstract
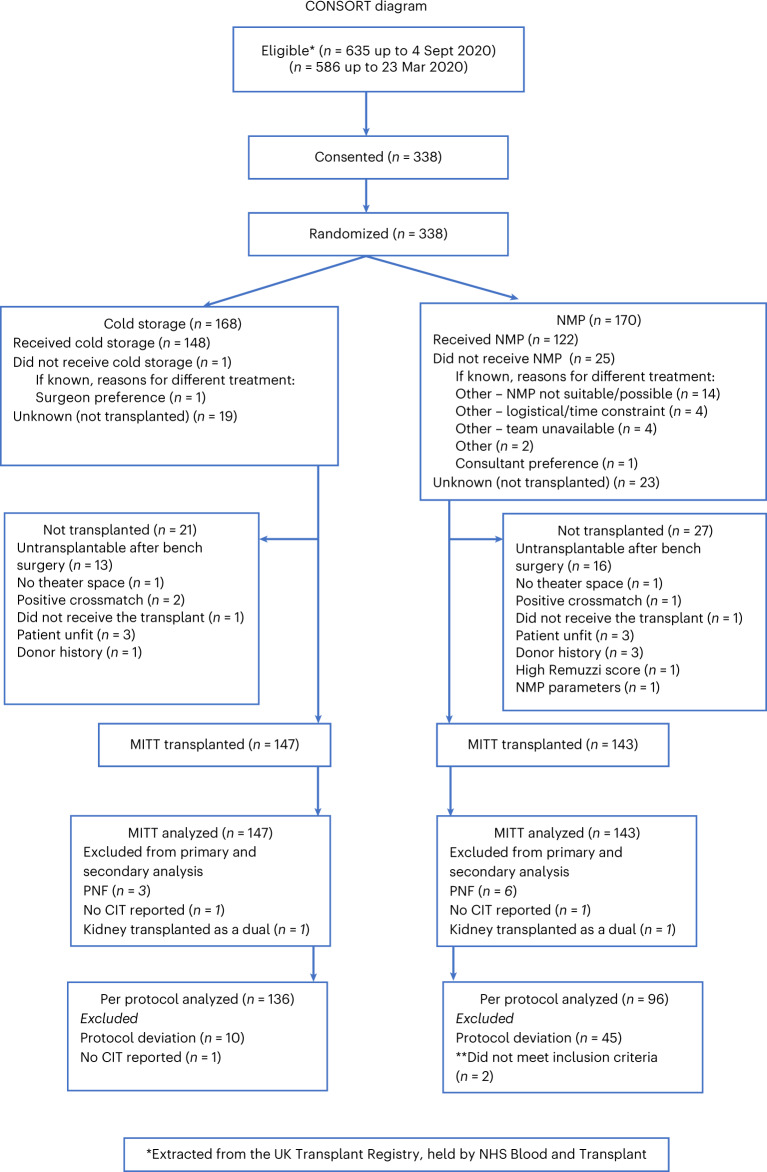
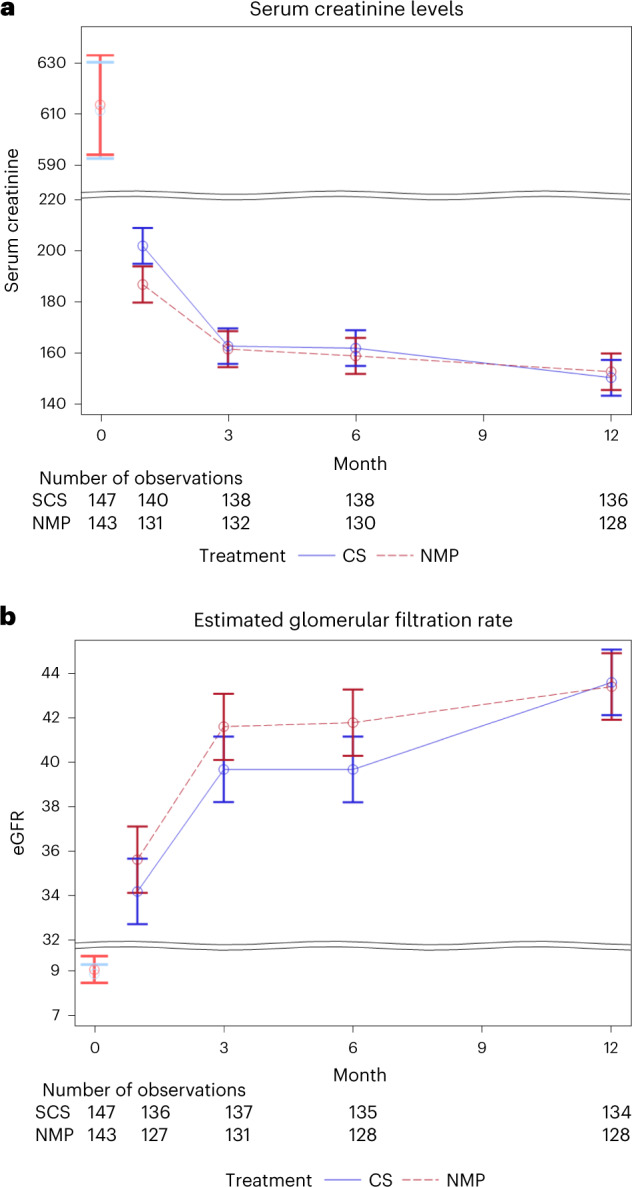
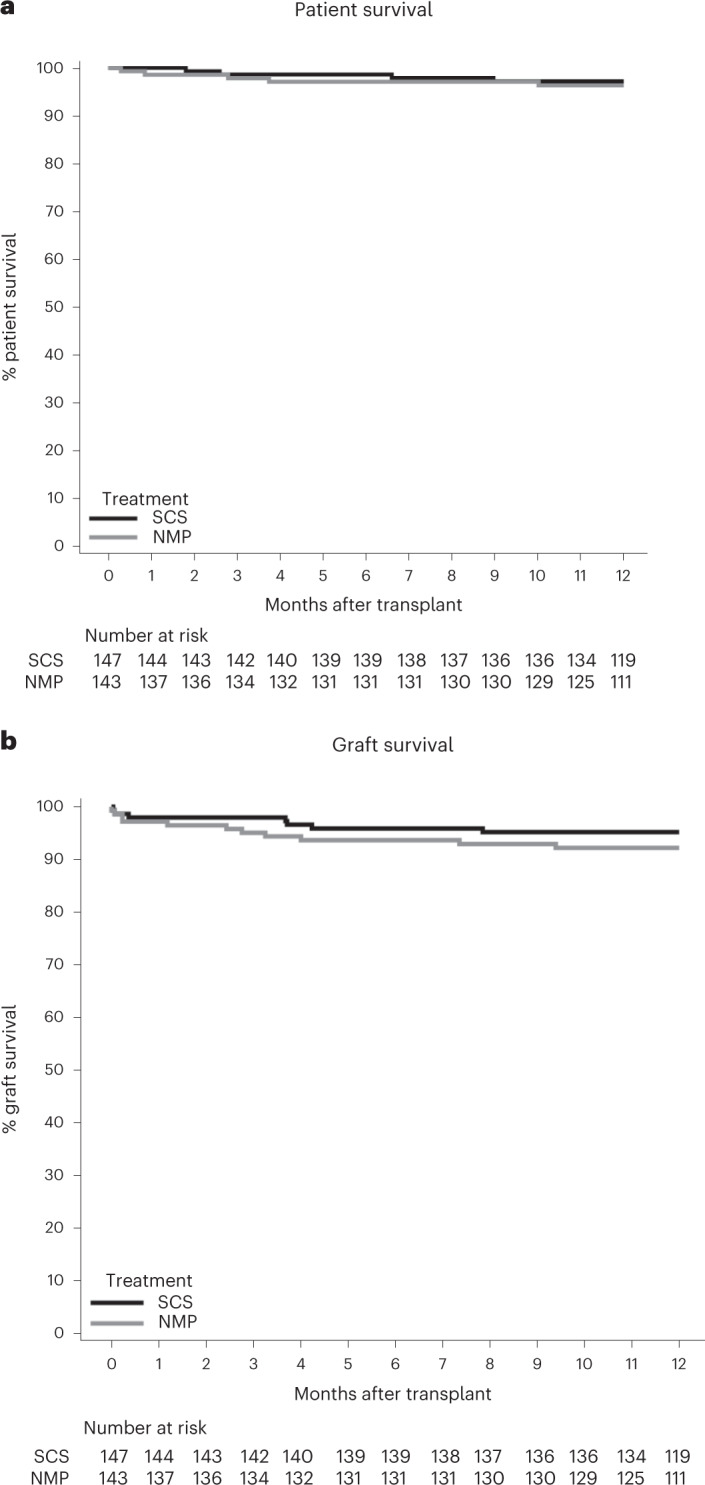
Kidney transplantation is the optimal treatment for end-stage renal disease, but it is still severely limited by a lack of suitable organ donors. Kidneys from donation after circulatory death (DCD) donors have been used to increase transplant rates, but these organs are susceptible to cold ischemic injury in the storage period before transplantation, the clinical consequence of which is high rates of delayed graft function (DGF). Normothermic machine perfusion (NMP) is an emerging technique that circulates a warmed, oxygenated red-cell-based perfusate through the kidney to maintain near-physiological conditions. We conducted a randomized controlled trial to compare the outcome of DCD kidney transplants after conventional static cold storage (SCS) alone or SCS plus 1-h NMP. A total of 338 kidneys were randomly allocated to SCS (n = 168) or NMP (n = 170), and 277 kidneys were included in the final intention-to-treat analysis. The primary endpoint was DGF, defined as the requirement for dialysis in the first 7 d after transplant. The rate of DGF was 82 of 135 (60.7%) in NMP kidneys versus 83 of 142 (58.5%) in SCS kidneys (adjusted odds ratio (95% confidence interval) 1.13 (0.69-1.84); P = 0.624). NMP was not associated with any increase in transplant thrombosis, infectious complications or any other adverse events. A 1-h period of NMP at the end of SCS did not reduce the rate of DGF in DCD kidneys. NMP was demonstrated to be feasible, safe and suitable for clinical application. Trial registration number: ISRCTN15821205 .
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
