

International practice patterns of dyslipidemia management in patients with chronic kidney disease under nephrology care: is it time to review guideline recommendations?
- PMID: 37231413
- PMCID: PMC10210460
- DOI: 10.1186/s12944-023-01833-z
International practice patterns of dyslipidemia management in patients with chronic kidney disease under nephrology care: is it time to review guideline recommendations?
Abstract
Background: In contrast to guidelines related to lipid therapy in other areas, 2012 Kidney Disease Improving Global Outcomes (KDIGO) guidelines recommend conducting a lipid profile upon diagnosis of chronic kidney disease (CKD) and treating all patients older than 50 years without defining a target for lipid levels. We evaluated multinational practice patterns for lipid management in patients with advanced CKD under nephrology care.
Methods: We analyzed lipid-lowering therapy (LLT), LDL- cholesterol (LDL-C) levels, and nephrologist-specified LDL-C goal upper limits in adult patients with eGFR < 60 ml/min from nephrology clinics in Brazil, France, Germany, and the United States (2014-2019). Models were adjusted for CKD stage, country, cardiovascular risk indicators, sex, and age.
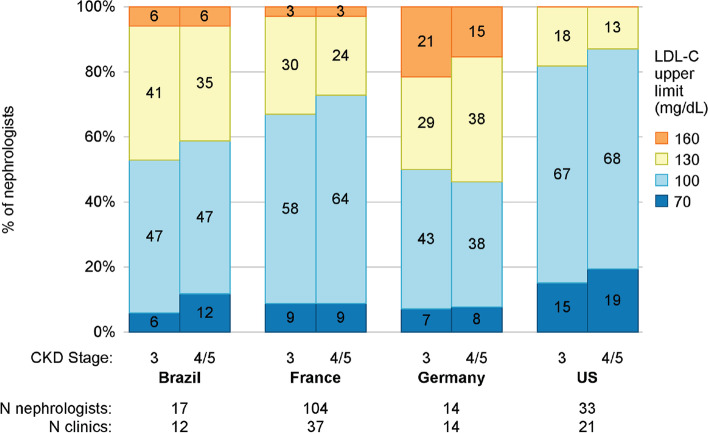
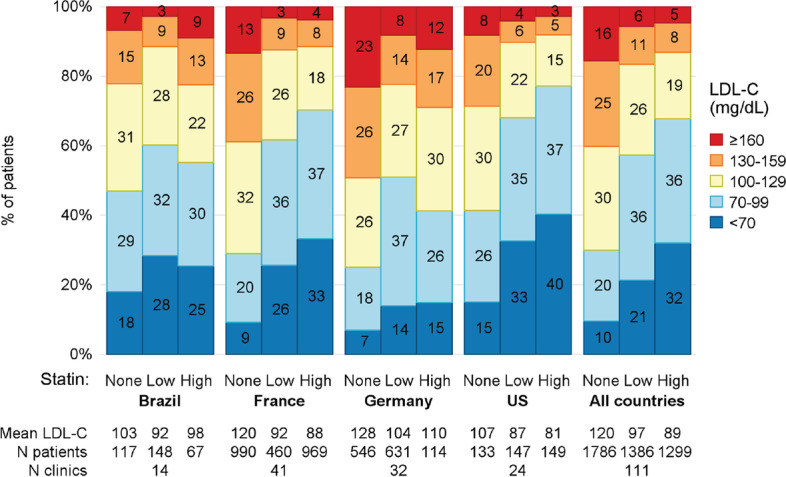
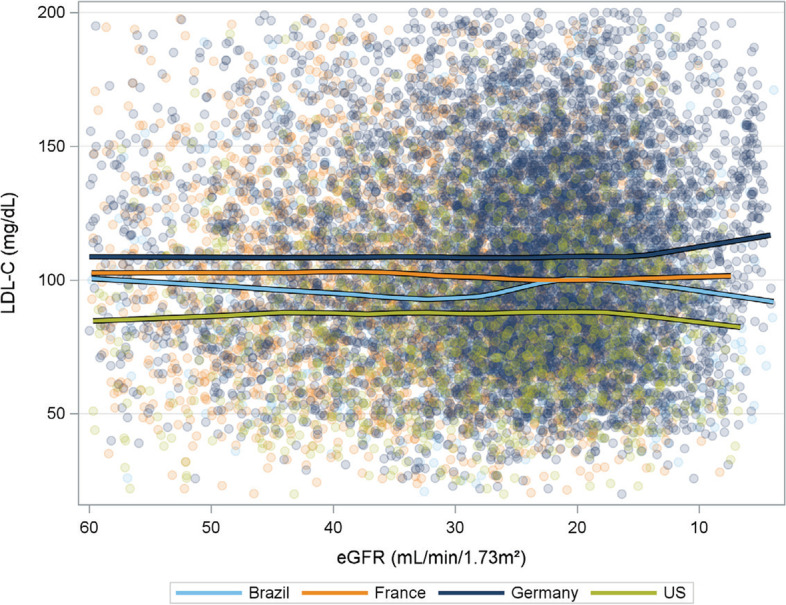
Results: LLT treatment differed significantly by country, from 51% in Germany to 61% in the US and France (p = 0.002) for statin monotherapy. For ezetimibe with or without statins, the prevalence was 0.3% in Brazil to 9% in France (< 0.001). Compared with patients not taking lipid-lowering therapy, LDL-C was lower among treated patients (p < 0.0001) and differed significantly by country (p < 0.0001). At the patient level, the LDL-C levels and statin prescription did not vary significantly by CKD stage (p = 0.09 LDL-C and p = 0.24 statin use). Between 7-23% of untreated patients in each country had LDL-C ≥ 160 mg/dL. Only 7-17% of nephrologists believed that LDL-C should be < 70 mg/dL.
Conclusion: There is substantial variation in practice patterns regarding LLT across countries but not across CKD stages. Treated patients appear to benefit from LDL-C lowering, yet a significant proportion of hyperlipidemia patients under nephrologist care are not receiving treatment.
Keywords: Chronic kidney disease; Dyslipidemia; LDL-C; Lipids management; Statins.
© 2023. The Author(s).
Conflict of interest statement
This manuscript was directly supported by Amgen. Global support for the ongoing DOPPS Programs is provided without restriction on publications by a variety of funders. For details see
Figures

References
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Lipid Work Group. KDIGO clinical practice guideline for lipid management in chronic kidney disease. Kidney Int Suppl. 2013;3(3):259-305.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
