

The Effect of Lung Resection for NSCLC on Circulating Immune Cells: A Pilot Study
- PMID: 37232845
- PMCID: PMC10217048
- DOI: 10.3390/curroncol30050387
The Effect of Lung Resection for NSCLC on Circulating Immune Cells: A Pilot Study
Abstract
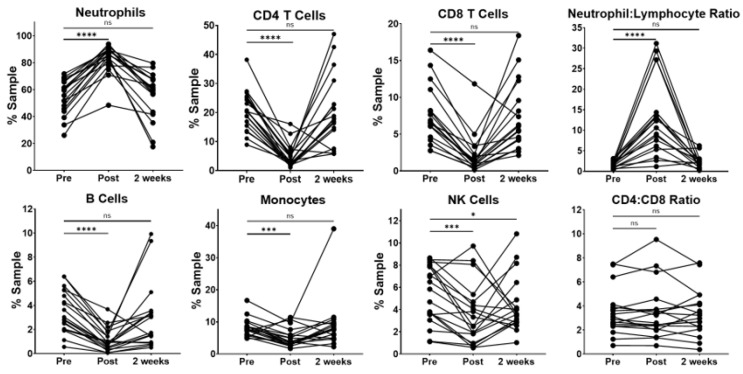
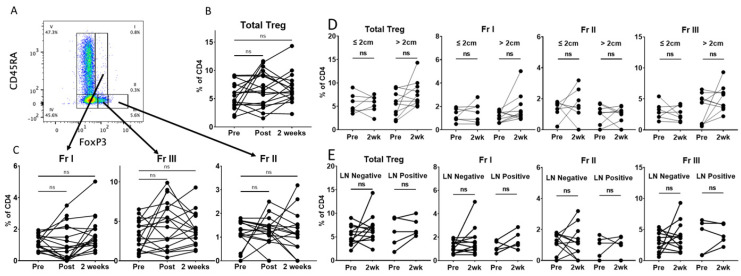
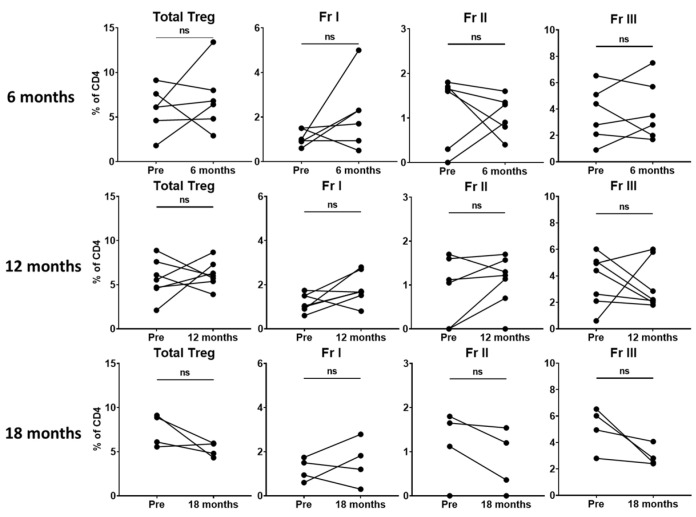
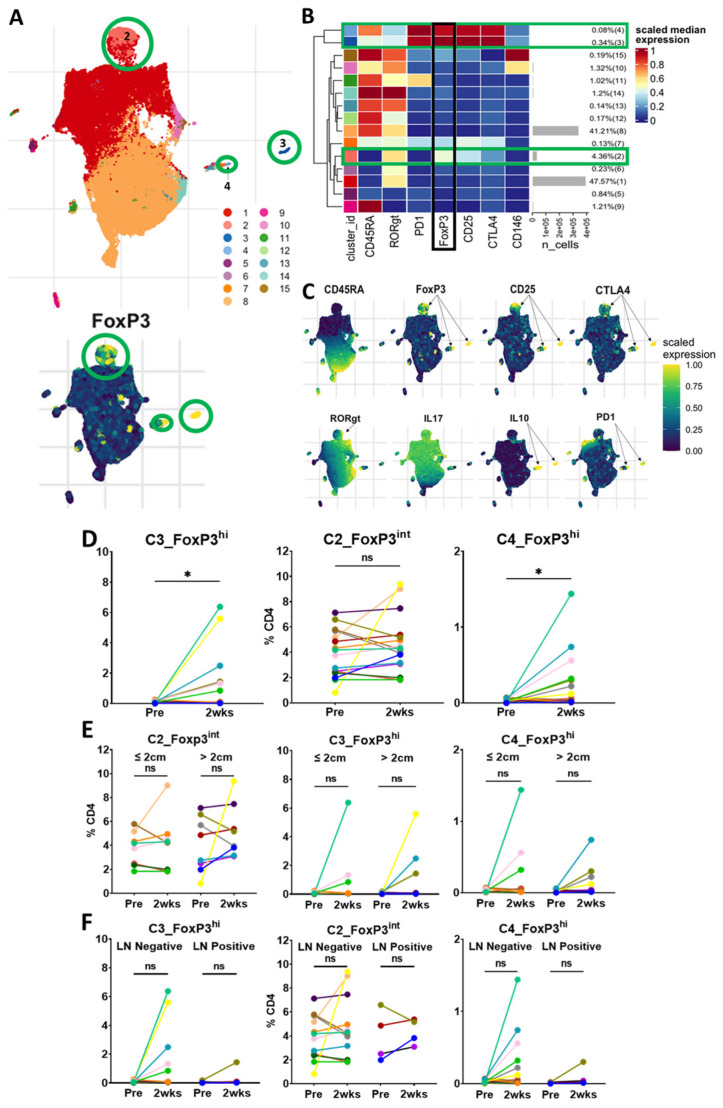
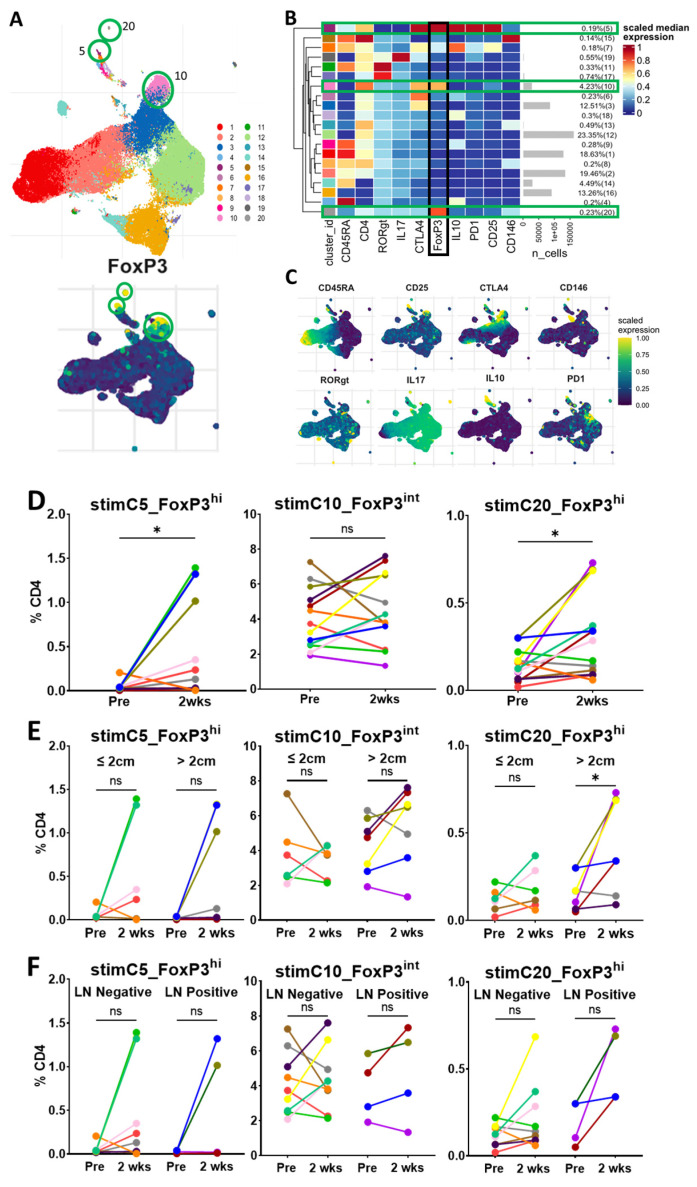
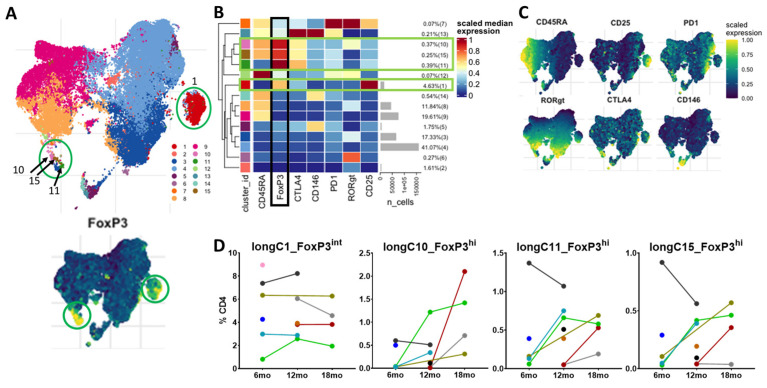
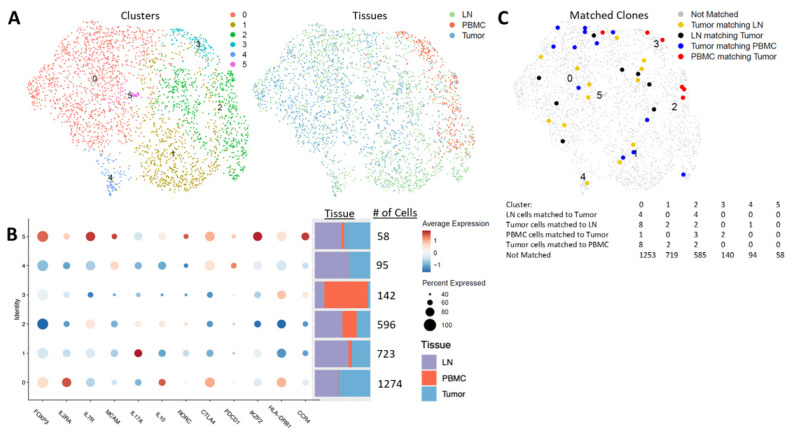
This pilot study sought to evaluate the circulating levels of immune cells, particularly regulatory T-cell (Treg) subsets, before and after lung resection for non-small cell lung cancer. Twenty-five patients consented and had specimens collected. Initially, peripheral blood of 21 patients was collected for circulating immune cell studies. Two of these patients were excluded due to technical issues, leaving 19 patients for the analyses of circulating immune cells. Standard gating and high-dimensional unsupervised clustering flow cytometry analyses were performed. The blood, tumors and lymph nodes were analyzed via single-cell RNA and TCR sequencing for Treg analyses in a total of five patients (including four additional patients from the initial 21 patients). Standard gating flow cytometry revealed a transient increase in neutrophils immediately following surgery, with a variable neutrophil-lymphocyte ratio and a stable CD4-CD8 ratio. Unexpectedly, the total Treg and Treg subsets did not change with surgery with standard gating in short- or long-term follow-up. Similarly, unsupervised clustering of Tregs revealed a dominant cluster that was stable perioperatively and long-term. Two small FoxP3hi clusters slightly increased following surgery. In the longer-term follow-up, these small FoxP3hi Treg clusters were not identified, indicating that they were likely a response to surgery. Single-cell sequencing demonstrated six CD4+FoxP3+ clusters among the blood, tumors and lymph nodes. These clusters had a variable expression of FoxP3, and several were mainly, or only, present in tumor and lymph node tissue. As such, serial monitoring of circulating Tregs may be informative, but not completely reflective of the Tregs present in the tumor microenvironment.
Keywords: Treg subsets; circulating immune cells; lung resection; non-small cell lung cancer; regulatory T cells; single-cell sequencing.
Conflict of interest statement
The authors declare no conflict of interest that may be perceived as inappropriately influencing the representation or interpretation of the reported research results. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results. JDP receives research support from KSQ Therapeutics, Inc. that is not related to the published work.
Figures
References
-
- World Health Organisation Cancer. [(accessed on 18 May 2021)]. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
