

Severe Hypertriglyceridaemia and Chylomicronaemia Syndrome-Causes, Clinical Presentation, and Therapeutic Options
- PMID: 37233662
- PMCID: PMC10224445
- DOI: 10.3390/metabo13050621
Severe Hypertriglyceridaemia and Chylomicronaemia Syndrome-Causes, Clinical Presentation, and Therapeutic Options
Abstract
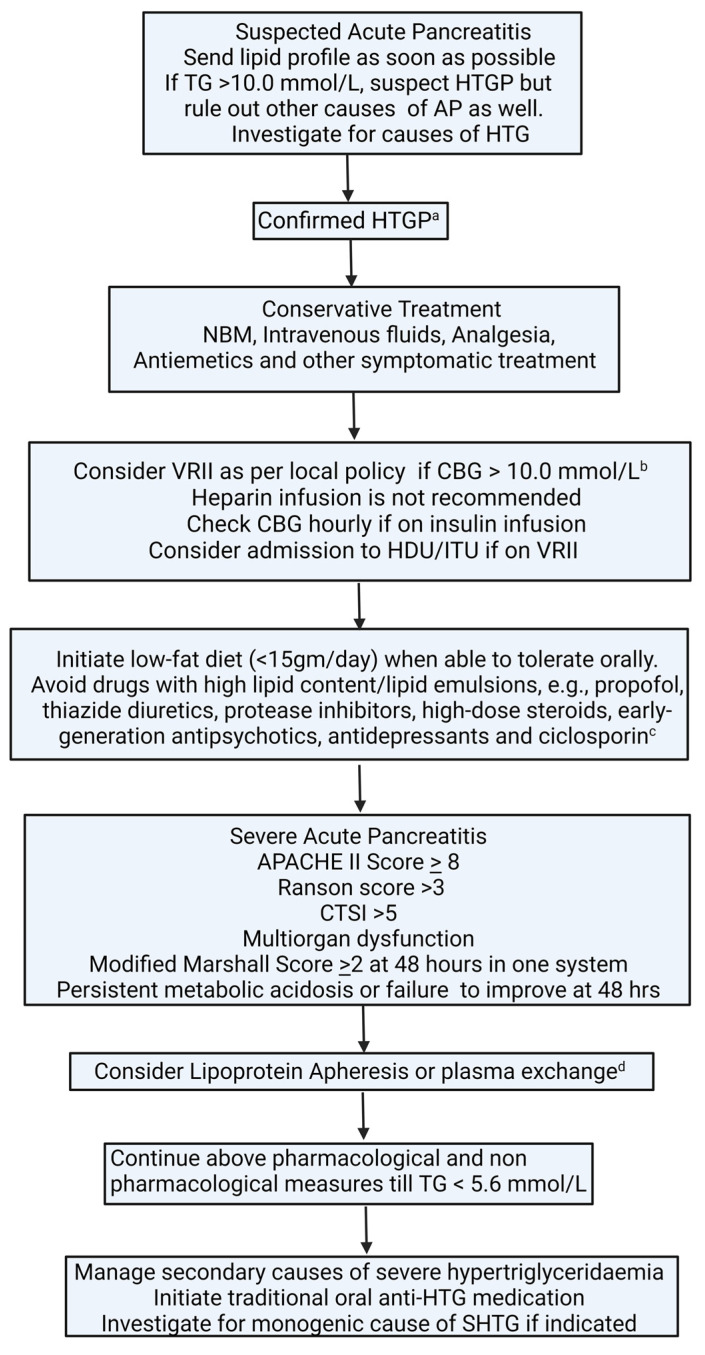
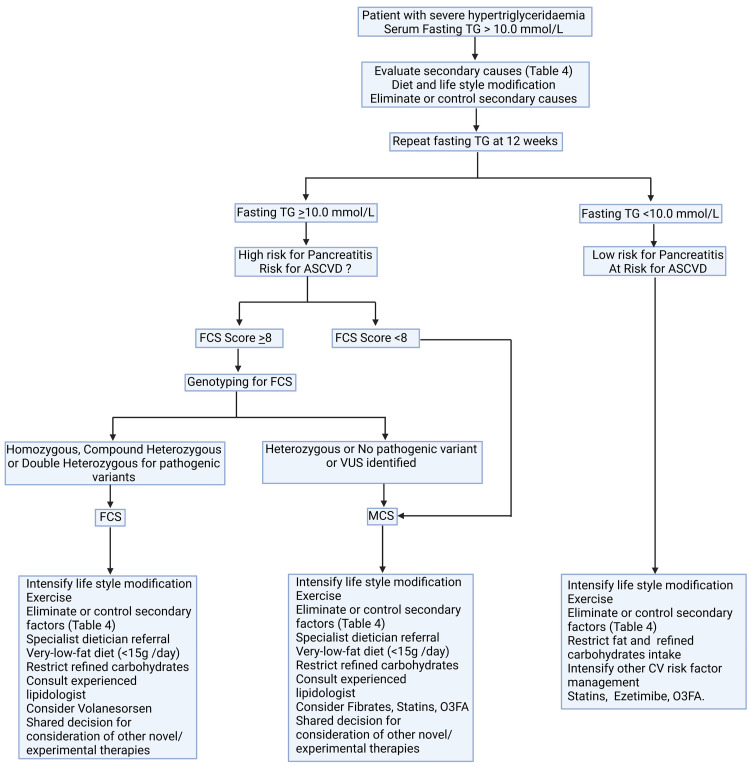
We have reviewed the genetic basis of chylomicronaemia, the difference between monogenic and polygenic hypertriglyceridaemia, its effects on pancreatic, cardiovascular, and microvascular complications, and current and potential future pharmacotherapies. Severe hypertriglyceridaemia (TG > 10 mmol/L or 1000 mg/dL) is rare with a prevalence of <1%. It has a complex genetic basis. In some individuals, the inheritance of a single rare variant with a large effect size leads to severe hypertriglyceridaemia and fasting chylomicronaemia of monogenic origin, termed as familial chylomicronaemia syndrome (FCS). Alternatively, the accumulation of multiple low-effect variants causes polygenic hypertriglyceridaemia, which increases the tendency to develop fasting chylomicronaemia in presence of acquired factors, termed as multifactorial chylomicronaemia syndrome (MCS). FCS is an autosomal recessive disease characterized by a pathogenic variant of the lipoprotein lipase (LPL) gene or one of its regulators. The risk of pancreatic complications and associated morbidity and mortality are higher in FCS than in MCS. FCS has a more favourable cardiometabolic profile and a low prevalence of atherosclerotic cardiovascular disease (ASCVD) compared to MCS. The cornerstone of the management of severe hypertriglyceridaemia is a very-low-fat diet. FCS does not respond to traditional lipid-lowering therapies. Several novel pharmacotherapeutic agents are in various phases of development. Data on the correlation between genotype and phenotype in FCS are scarce. Further research to investigate the impact of individual gene variants on the natural history of the disease, and its link with ASCVD, microvascular disease, and acute or recurrent pancreatitis, is warranted. Volanesorsen reduces triglyceride concentration and frequency of pancreatitis effectively in patients with FCS and MCS. Several other therapeutic agents are in development. Understanding the natural history of FCS and MCS is necessary to rationalise healthcare resources and decide when to deploy these high-cost low-volume therapeutic agents.
Keywords: atherosclerosis; chylomicronaemia syndrome; hypertriglyceridaemia; microvascular complications; pancreatitis; volanesorsen.
Conflict of interest statement
P.D.: received honoraria for speaking from Amgen, Daichii-Sanko, Novartis, and Sobi Pharmaceuticals. P.H.: received speaking honoraria from Amgen and participated on an Advisory Board for Daiichi Sankyo. G.F.: received scientific expert fees from the European Food Safety Agency, a speaker fee from Daiichi Sankyo, and funding from Sanofi. Member of Medical, Scientific and Research Committee HEART UK. D.D.: member of advisory boards and speaker for Sobi and Ackea. A.W.: site investigator for volanesorsen and evanicumab in FCS and received grants from Akcea and Regeneron. H.D.: clinical advisor to the ERG report commissioned by the NIHR HTA Programme. H.S.: received personal fees from Amgen, Akcea, Synageva, NAPP, Novartis, Takeda, Sanofi, Pfizer, and Kowa and research grants and donations from Akcea, Pfizer, MSD, Amgen, Genzyme-Sanofi, Synageva, Amryt, Synageva, and Alexion. J.C., C.D., F.J., M.M., Y.T., P.N.D., Z.M., H.H., J.H., B.B.: No conflicts of interest.
Figures
References
-
- Virani S.S., Morris P.B., Agarwala A., Ballantyne C.M., Birtcher K.K., Kris-Etherton P.M., Stone N.J. 2021 ACC Expert Consensus Decision Pathway on the Management of ASCVD Risk Reduction in Patients with Persistent Hypertriglyceridemia: A Report of the American College of Car-diology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2021;78:960–993. doi: 10.1016/j.jacc.2021.06.011. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
