

Genome-wide association analysis identifies ancestry-specific genetic variation associated with acute response to metformin and glipizide in SUGAR-MGH
- PMID: 37233759
- PMCID: PMC10790310
- DOI: 10.1007/s00125-023-05922-7
Genome-wide association analysis identifies ancestry-specific genetic variation associated with acute response to metformin and glipizide in SUGAR-MGH
Abstract
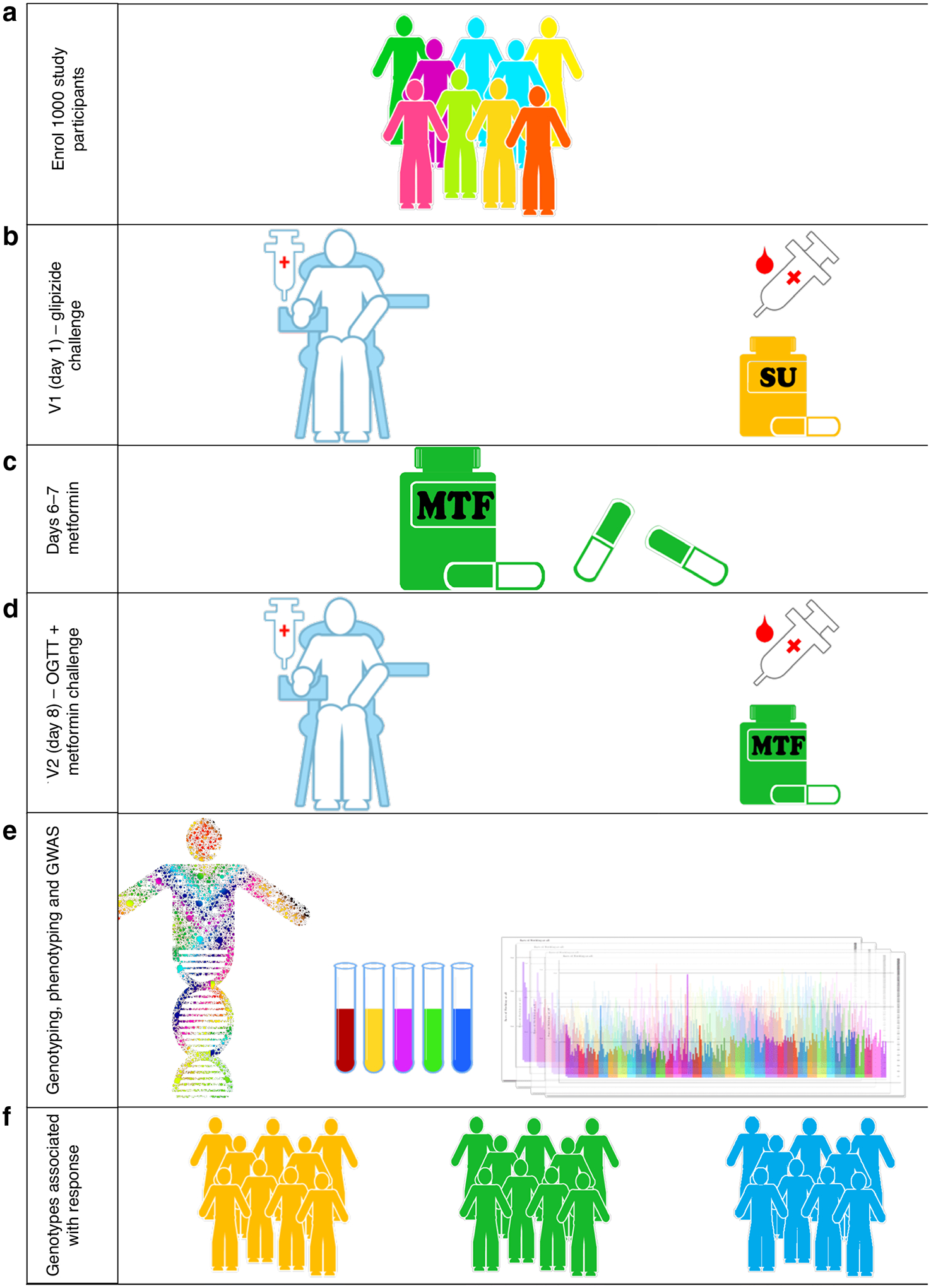
Aims/hypothesis: Characterisation of genetic variation that influences the response to glucose-lowering medications is instrumental to precision medicine for treatment of type 2 diabetes. The Study to Understand the Genetics of the Acute Response to Metformin and Glipizide in Humans (SUGAR-MGH) examined the acute response to metformin and glipizide in order to identify new pharmacogenetic associations for the response to common glucose-lowering medications in individuals at risk of type 2 diabetes.
Methods: One thousand participants at risk for type 2 diabetes from diverse ancestries underwent sequential glipizide and metformin challenges. A genome-wide association study was performed using the Illumina Multi-Ethnic Genotyping Array. Imputation was performed with the TOPMed reference panel. Multiple linear regression using an additive model tested for association between genetic variants and primary endpoints of drug response. In a more focused analysis, we evaluated the influence of 804 unique type 2 diabetes- and glycaemic trait-associated variants on SUGAR-MGH outcomes and performed colocalisation analyses to identify shared genetic signals.
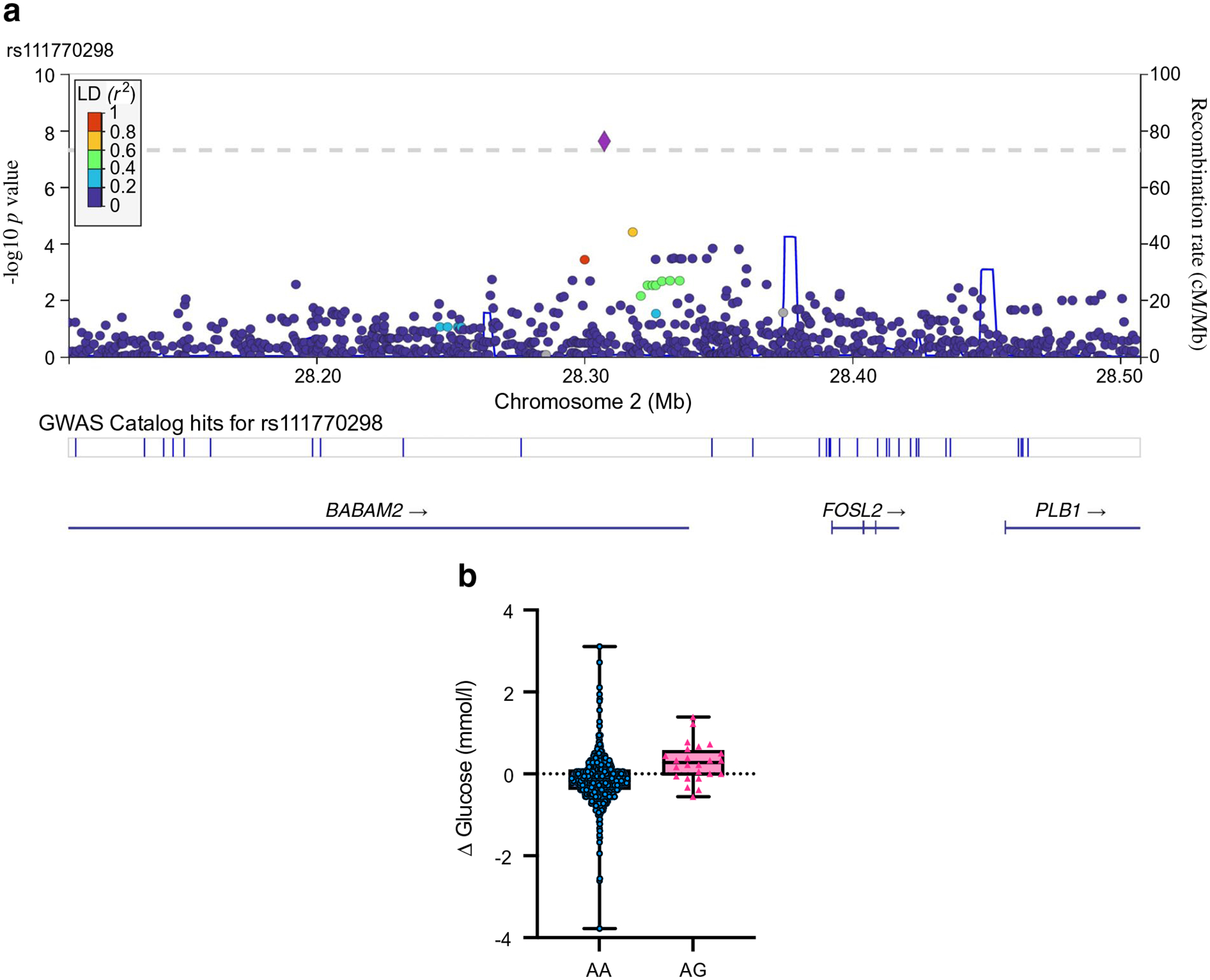
Results: Five genome-wide significant variants were associated with metformin or glipizide response. The strongest association was between an African ancestry-specific variant (minor allele frequency [MAFAfr]=0.0283) at rs149403252 and lower fasting glucose at Visit 2 following metformin (p=1.9×10-9); carriers were found to have a 0.94 mmol/l larger decrease in fasting glucose. rs111770298, another African ancestry-specific variant (MAFAfr=0.0536), was associated with a reduced response to metformin (p=2.4×10-8), where carriers had a 0.29 mmol/l increase in fasting glucose compared with non-carriers, who experienced a 0.15 mmol/l decrease. This finding was validated in the Diabetes Prevention Program, where rs111770298 was associated with a worse glycaemic response to metformin: heterozygous carriers had an increase in HbA1c of 0.08% and non-carriers had an HbA1c increase of 0.01% after 1 year of treatment (p=3.3×10-3). We also identified associations between type 2 diabetes-associated variants and glycaemic response, including the type 2 diabetes-protective C allele of rs703972 near ZMIZ1 and increased levels of active glucagon-like peptide 1 (GLP-1) (p=1.6×10-5), supporting the role of alterations in incretin levels in type 2 diabetes pathophysiology.
Conclusions/interpretation: We present a well-phenotyped, densely genotyped, multi-ancestry resource to study gene-drug interactions, uncover novel variation associated with response to common glucose-lowering medications and provide insight into mechanisms of action of type 2 diabetes-related variation.
Data availability: The complete summary statistics from this study are available at the Common Metabolic Diseases Knowledge Portal ( https://hugeamp.org ) and the GWAS Catalog ( www.ebi.ac.uk/gwas/ , accession IDs: GCST90269867 to GCST90269899).
Keywords: Genetics; Genome-wide association study; Glipizide; Incretin; Metformin; Multi-ancestry; Pathophysiology; Pharmacogenetics; Sulfonylurea; Type 2 diabetes.
© 2023. The Author(s), under exclusive licence to Springer-Verlag GmbH Germany, part of Springer Nature.
Figures

References
-
- Srinivasan S, Kaur V, Chamarthi B et al. (2018) TCF7L2 Genetic variation augments incretin resistance and influences response to a sulfonylurea and metformin: the study to understand the genetics of the acute response to Metformin and Glipizide in Humans (SUGAR-MGH). Diabetes Care 41(3):554–561. 10.2337/dc17-1386 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MC_UU_00007/10/MRC_/Medical Research Council/United Kingdom
- MC_UU_00033/3/MRC_/Medical Research Council/United Kingdom
- T32 DK007028/DK/NIDDK NIH HHS/United States
- K23 DK114551/DK/NIDDK NIH HHS/United States
- MC_PC_14089/MRC_/Medical Research Council/United Kingdom
- MR/M009203/1/MRC_/Medical Research Council/United Kingdom
- S10 OD026880/OD/NIH HHS/United States
- P30 DK036836/DK/NIDDK NIH HHS/United States
- M01 RR001066/RR/NCRR NIH HHS/United States
- R01 DK088214/DK/NIDDK NIH HHS/United States
- U01 HG011723/HG/NHGRI NIH HHS/United States
- R01 GM117163/DK/NIDDK NIH HHS/United States
- S10 OD030463/OD/NIH HHS/United States
- UL1 TR000170/TR/NCATS NIH HHS/United States
- K23 DK131345/DK/NIDDK NIH HHS/United States
- U01 DK048377/DK/NIDDK NIH HHS/United States
- P30 ES010126/ES/NIEHS NIH HHS/United States
- MR/R024227/1/MRC_/Medical Research Council/United Kingdom
- R03 DK077675/DK/NIDDK NIH HHS/United States
- R01 HD030880/HD/NICHD NIH HHS/United States
- MC_EX_MR/M009203/1/MRC_/Medical Research Council/United Kingdom
- MC_UU_00033/1/MRC_/Medical Research Council/United Kingdom
- UL1 RR025758/RR/NCRR NIH HHS/United States
- R01 GM117163/GM/NIGMS NIH HHS/United States
- MR/R010676/1/MRC_/Medical Research Council/United Kingdom
- K23 DK125839/DK/NIDDK NIH HHS/United States
- K24 HL157960/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
