

Low circulating adropin concentrations predict increased risk of cognitive decline in community-dwelling older adults
- PMID: 37233882
- PMCID: PMC10828274
- DOI: 10.1007/s11357-023-00824-3
Low circulating adropin concentrations predict increased risk of cognitive decline in community-dwelling older adults
Abstract
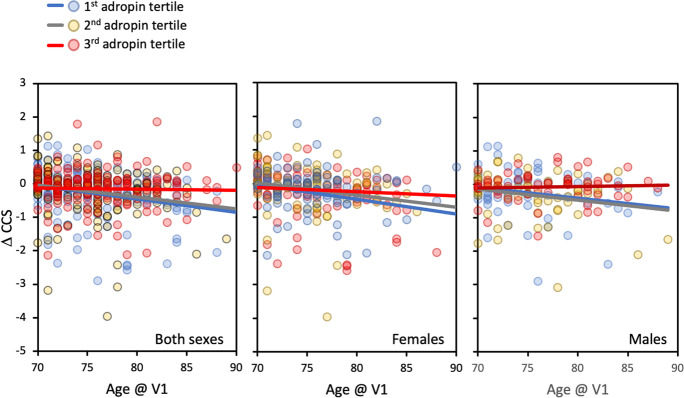
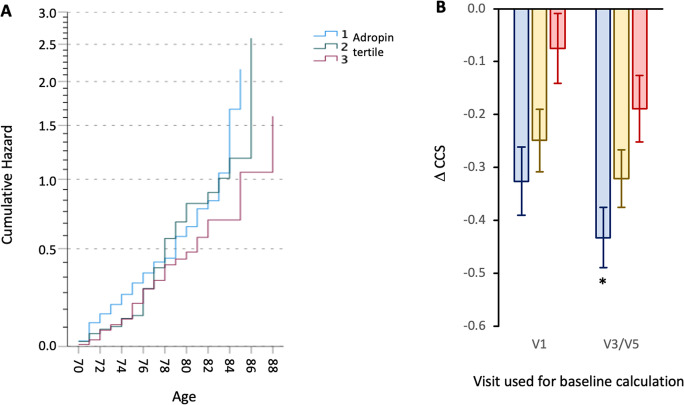
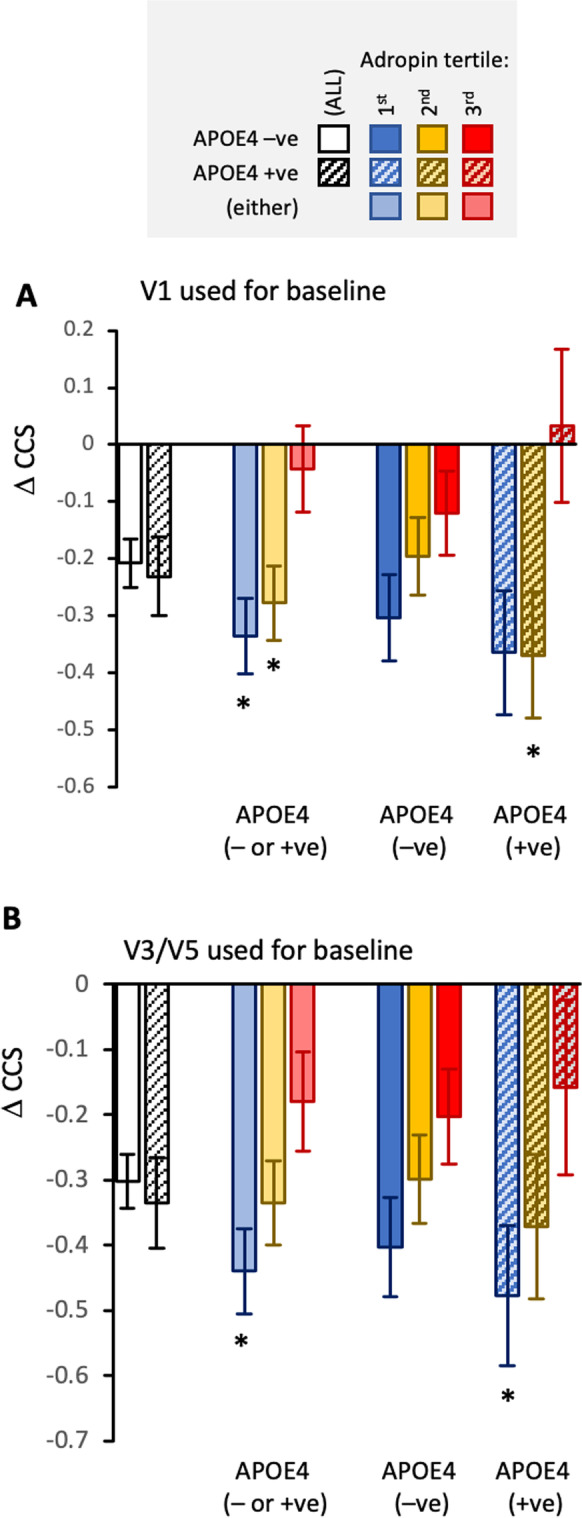
The secreted peptide adropin is highly expressed in human brain tissues and correlates with RNA and proteomic risk indicators for dementia. Here we report that plasma adropin concentrations predict risk for cognitive decline in the Multidomain Alzheimer Preventive Trial (ClinicalTrials.gov Identifier, NCT00672685; mean age 75.8y, SD = 4.5 years, 60.2% female, n = 452). Cognitive ability was evaluated using a composite cognitive score (CCS) that assessed four domains: memory, language, executive function, and orientation. Relationships between plasma adropin concentrations and changes in CCS (∆CCS) were examined using Cox Proportional Hazards Regression, or by grouping into tertiles ranked low to high by adropin values and controlling for age, time between baseline and final visits, baseline CCS, and other risk factors (e.g., education, medication, APOE4 status). Risk of cognitive decline (defined as a ∆CCS of - 0.3 or more) decreased with increasing plasma adropin concentrations (hazard ratio = 0.873, 95% CI 0.780-0.977, P = 0.018). Between adropin tertiles, ∆CCS was significantly different (P = 0.01; estimated marginal mean ± SE for the 1st to 3rd tertile, - 0.317 ± 0.064; - 0.275 ± 0.063; - 0.042 ± 0.071; n = 133,146, and 130, respectively; P < 0.05 for 1st vs. 2nd and 3rd adropin tertiles). Normalized plasma Aß42/40 ratio and plasma neurofilament light chain, indicators of neurodegeneration, were significantly different between adropin tertile. These differences were consistent with reduced risk of cognitive decline with higher plasma adropin levels. Overall, these results suggest cognitive decline is reduced in community-dwelling older adults with higher circulating adropin levels. Further studies are needed to determine the underlying causes of the relationship and whether increasing adropin levels can delay cognitive decline.
Keywords: Adropin; Aging; Cognitive decline; Dementia; Plasma biomarkers.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Alzheimer's Association Report. Alzheimer’s disease facts and figures. Alzheimers Dement. 2023;19(4):1598–695. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
