

Increasing the Passive Range of Joint Motion in Stroke Patients Using Botulinum Toxin: The Role of Pain Relief
- PMID: 37235369
- PMCID: PMC10223867
- DOI: 10.3390/toxins15050335
Increasing the Passive Range of Joint Motion in Stroke Patients Using Botulinum Toxin: The Role of Pain Relief
Abstract
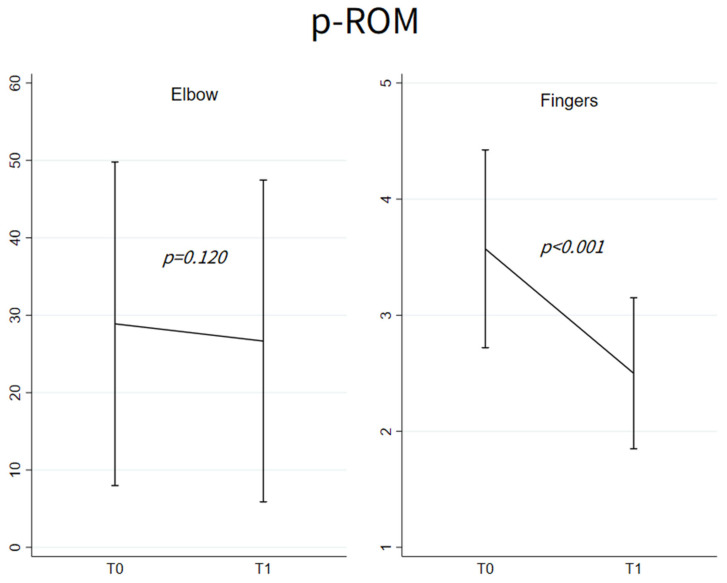
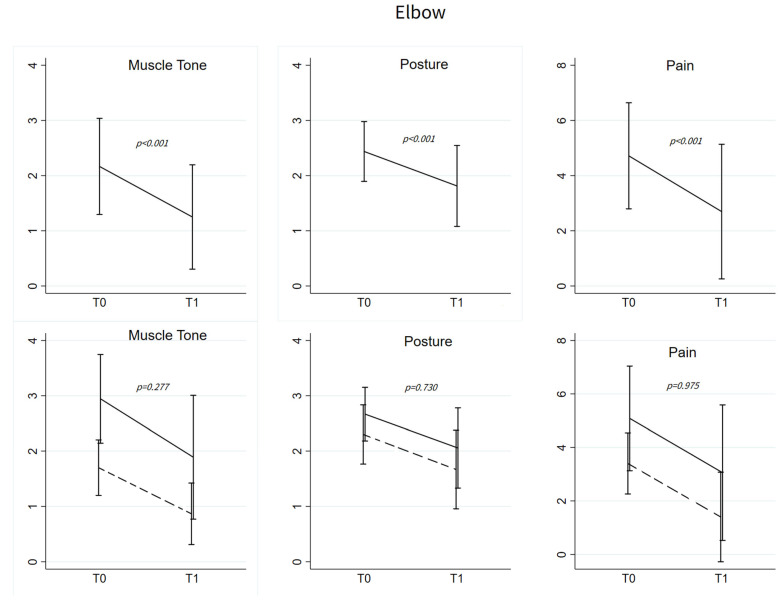
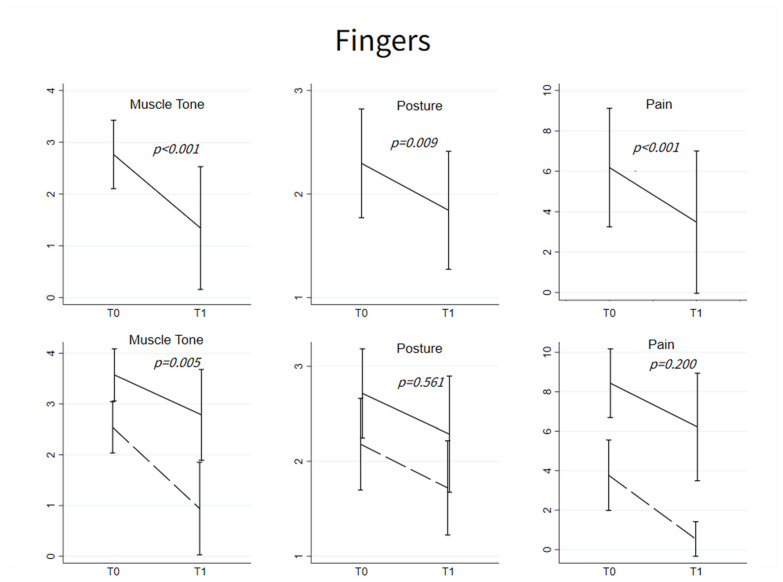
By blocking the release of neurotransmitters, botulinum toxin A (BoNT-A) is an effective treatment for muscle over-activity and pain in stroke patients. BoNT-A has also been reported to increase passive range of motion (p-ROM), the decrease of which is mainly due to muscle shortening (i.e., muscle contracture). Although the mechanism of action of BoNT-A on p-ROM is far from understood, pain relief may be hypothesized to play a role. To test this hypothesis, a retrospective investigation of p-ROM and pain was conducted in post-stroke patients treated with BoNT-A for upper limb hypertonia. Among 70 stroke patients enrolled in the study, muscle tone (Modified Ashworth Scale), pathological postures, p-ROM, and pain during p-ROM assessment (Numeric Rating Scale, NRS) were investigated in elbow flexors (48 patients) and in finger flexors (64 patients), just before and 3-6 weeks after BoNT-A treatment. Before BoNT-A treatment, pathological postures of elbow flexion were found in all patients but one. A decreased elbow p-ROM was found in 18 patients (38%). Patients with decreased p-ROM had higher pain-NRS scores (5.08 ± 1.96, with a pain score ≥8 in 11% of cases) than patients with normal p-ROM (0.57 ± 1.36) (p < 0.001). Similarly, pathological postures of finger flexion were found in all patients but two. A decreased finger p-ROM was found in 14 patients (22%). Pain was more intense in the 14 patients with decreased p-ROM (8.43 ± 1.74, with a pain score ≥ 8 in 86% of cases) than in the 50 patients with normal p-ROM (0.98 ± 1.89) (p < 0.001). After BoNT-A treatment, muscle tone, pathological postures, and pain decreased in both elbow and finger flexors. In contrast, p-ROM increased only in finger flexors. The study discusses that pain plays a pivotal role in the increase in p-ROM observed after BoNT-A treatment.
Keywords: limb postures; pathological postures; spastic dystonia; spasticity; stretch.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Frenkel-Toledo S., Solomon J.M., Shah A., Baniña M.C., Berman S., Soroker N., Liebermann D.G., Levin M.F. Tonic Stretch Reflex Threshold as a Measure of Spasticity after Stroke: Reliability, Minimal Detectable Change and Responsiveness. Clin. Neurophysiol. 2021;132:1226–1233. doi: 10.1016/j.clinph.2021.02.390. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
