

Diagnostic yield of pediatric and prenatal exome sequencing in a diverse population
- PMID: 37236975
- PMCID: PMC10220040
- DOI: 10.1038/s41525-023-00353-0
Diagnostic yield of pediatric and prenatal exome sequencing in a diverse population
Erratum in
-
Author Correction: Diagnostic yield of pediatric and prenatal exome sequencing in a diverse population.NPJ Genom Med. 2023 Oct 23;8(1):34. doi: 10.1038/s41525-023-00382-9. NPJ Genom Med. 2023. PMID: 37872195 Free PMC article. No abstract available.
Abstract
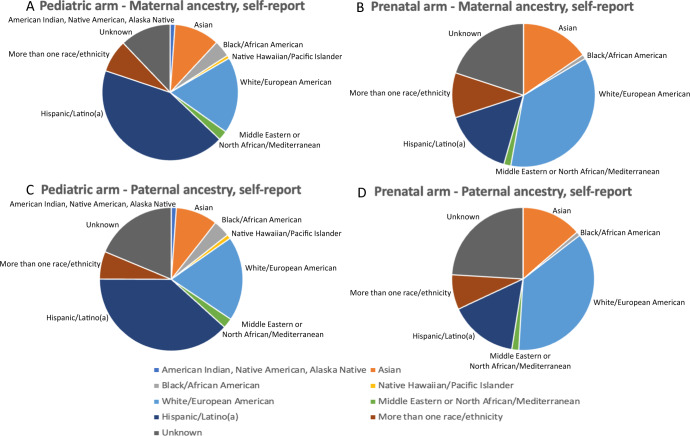
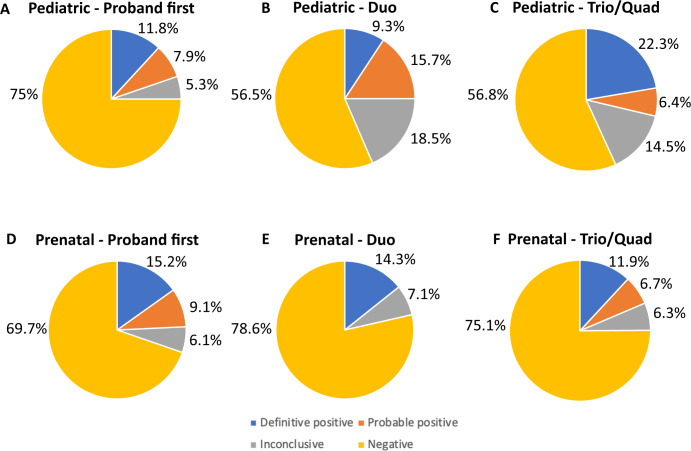
The diagnostic yield of exome sequencing (ES) has primarily been evaluated in individuals of European ancestry, with less focus on underrepresented minority (URM) and underserved (US) patients. We evaluated the diagnostic yield of ES in a cohort of predominantly US and URM pediatric and prenatal patients suspected to have a genetic disorder. Eligible pediatric patients had multiple congenital anomalies and/or neurocognitive disabilities and prenatal patients had one or more structural anomalies, disorders of fetal growth, or fetal effusions. URM and US patients were prioritized for enrollment and underwent ES at a single academic center. We identified definitive positive or probable positive results in 201/845 (23.8%) patients, with a significantly higher diagnostic rate in pediatric (26.7%) compared to prenatal patients (19.0%) (P = 0.01). For both pediatric and prenatal patients, the diagnostic yield and frequency of inconclusive findings did not differ significantly between URM and non-URM patients or between patients with US status and those without US status. Our results demonstrate a similar diagnostic yield of ES between prenatal and pediatric URM/US patients and non-URM/US patients for positive and inconclusive results. These data support the use of ES to identify clinically relevant variants in patients from diverse populations.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Adv. Exp. Med. Biol. 2010;686:349–364. - PubMed
-
- Alwan A, Modell B. Recommendations for introducing genetics services in developing countries. Nat. Rev. Genet. 2003;4:61–68. - PubMed
-
- Christianson A, Modell B. Medical genetics in developing countries. Annu Rev. Genomics Hum. Genet. 2004;5:219–265. - PubMed
