

Abdominal perfusion pressure in critically ill cirrhotic patients: a prospective observational study
- PMID: 37237113
- PMCID: PMC10214359
- DOI: 10.1038/s41598-023-34367-6
Abdominal perfusion pressure in critically ill cirrhotic patients: a prospective observational study
Abstract
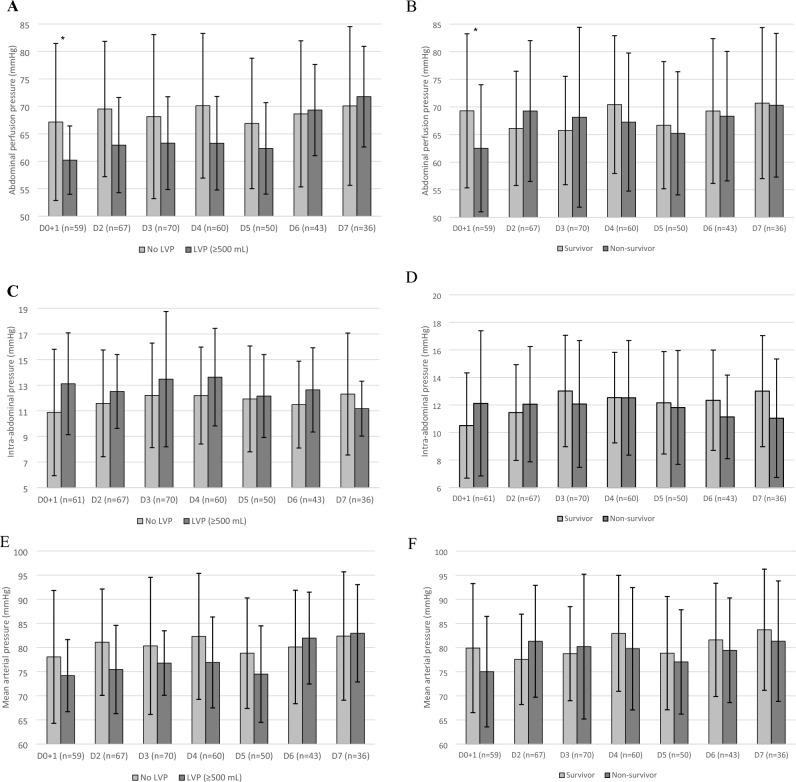
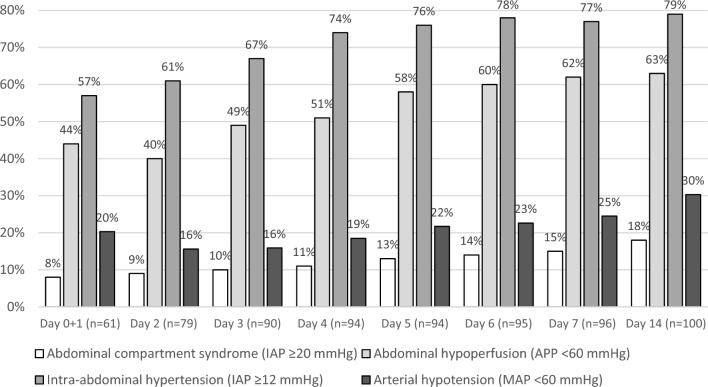
In critical patients, abdominal perfusion pressure (APP) has been shown to correlate with outcome. However, data from cirrhotic patients is scarce. We aimed to characterize APP in critically ill cirrhotic patients, analyze the prevalence and risk factors of abdominal hypoperfusion (AhP) and outcomes. A prospective cohort study in a general ICU specialized in liver disease at a tertiary hospital center recruited consecutive cirrhotic patients between October 2016 and December 2021. The study included 101 patients, with a mean age of 57.2 (± 10.4) years and a female gender proportion of 23.5%. The most frequent etiology of cirrhosis was alcohol (51.0%), and the precipitant event was infection (37.3%). ACLF grade (1-3) distribution was 8.9%, 26.7% and 52.5%, respectively. A total of 1274 measurements presented a mean APP of 63 (± 15) mmHg. Baseline AhP prevalence was 47%, independently associated with paracentesis (aOR 4.81, CI 95% 1.46-15.8, p = 0.01) and ACLF grade (aOR 2.41, CI 95% 1.20-4.85, p = 0.01). Similarly, AhP during the first week (64%) had baseline ACLF grade (aOR 2.09, CI 95% 1.29-3.39, p = 0.003) as a risk factor. Independent risk factors for 28-day mortality were bilirubin (aOR 1.10, CI 95% 1.04-1.16, p < 0.001) and SAPS II score (aOR 1.07, CI 95% 1.03-1.11, p = 0.001). There was a high prevalence of AhP in critical cirrhotic patients. Abdominal hypoperfusion was independently associated with higher ACLF grade and baseline paracentesis. Risk factors for 28-day mortality included clinical severity and total bilirubin. The prevention and treatment of AhP in the high-risk cirrhotic patient is prudential.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
