

Comparison of acute single versus multiple osteoporotic vertebral compression fractures in radiographic characteristic and bone fragility
- PMID: 37237306
- PMCID: PMC10224586
- DOI: 10.1186/s13018-023-03874-7
Comparison of acute single versus multiple osteoporotic vertebral compression fractures in radiographic characteristic and bone fragility
Abstract
Background: Osteoporotic vertebral compression fractures (OVCF) are common in aged population with bone fragility. This study aimed to identify the radiographic and bone fragility characteristic of acute single and multiple OVCF.
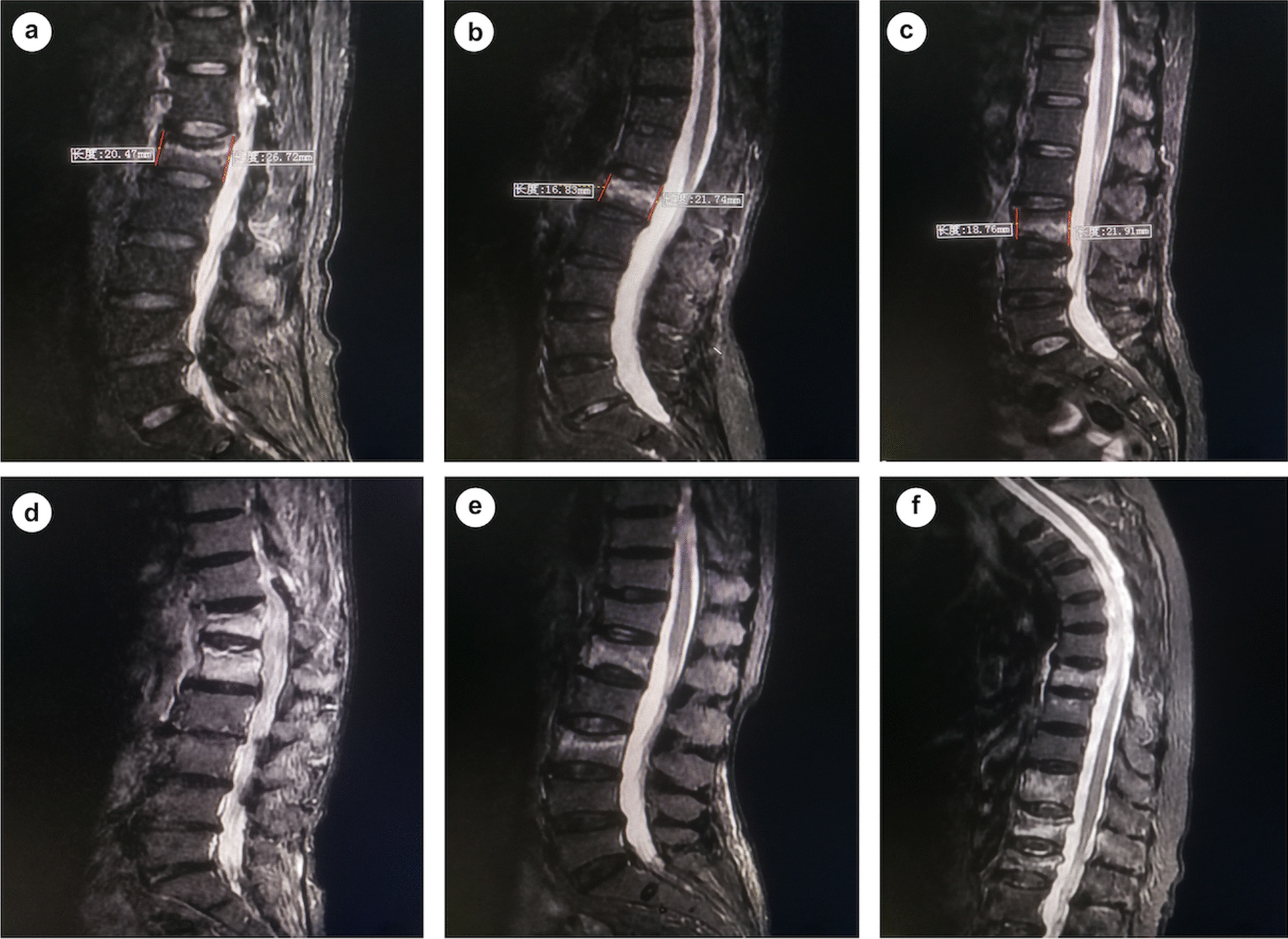
Methods: OVCF patients hospitalized in a spine center between June 2016 and October 2020 were retrospectively studied. Demographics, comorbidity, bone mineral density, spine trauma, duration of pre-hospital back pain, anatomical location and distribution pattern of OVCF, extent of vertebral marrow edema, and degree of vertebral compression of patients with multi-segment vertebral fractures (MSVF) were summarized and compared to those with single segment vertebral fractures (SSVF).
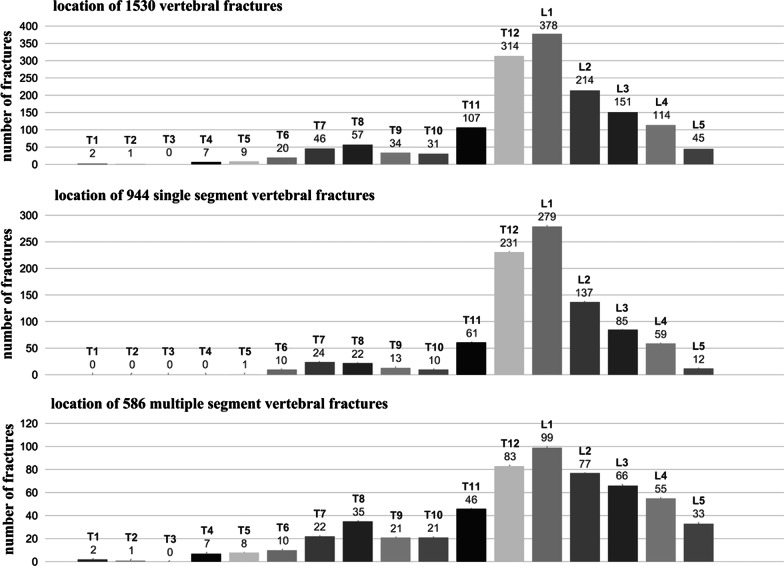
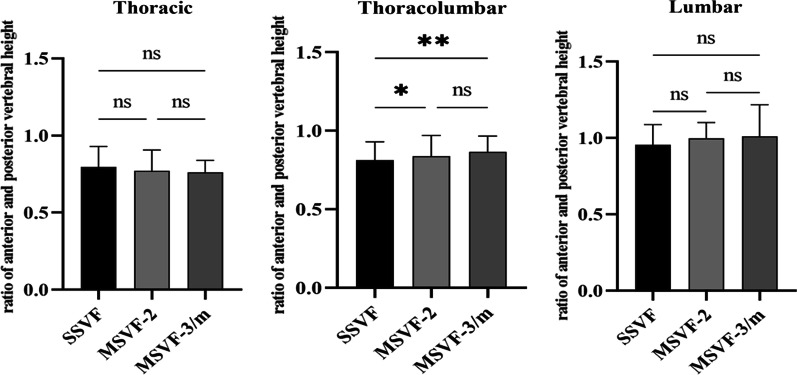
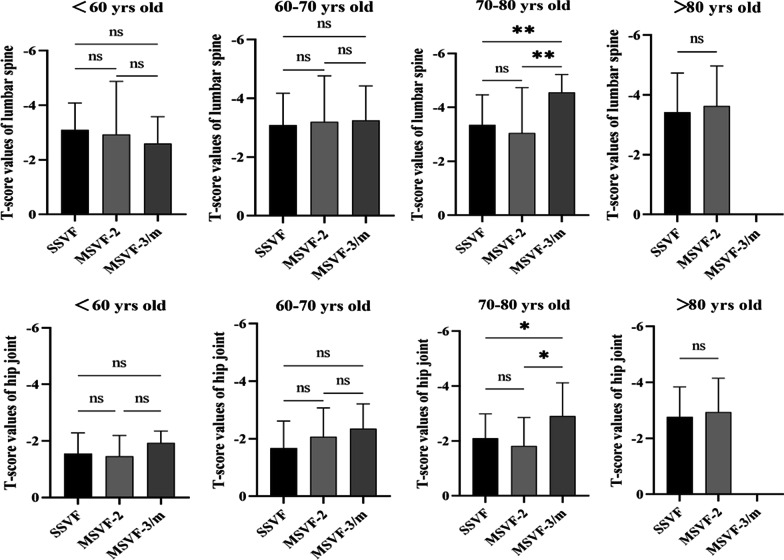
Results: A total of 1182 patients with 1530 acute fractured vertebrae were included. There were 944 SSVF (79.9%) and 238 MSVF (20.1%) simultaneously involving two (MSVF-2) or three and more vertebra (MSVF-3/m). The Female-Male ratio was 4.4 and differed not significantly between SSVF and MSVF. Females in SSVF were younger than males while MSVF-2 tended to occur in older females. L1, T12, and L2 were the three most frequently fractured vertebra and MSVF involved more vertebra in thoracic and lumbar spine. 31.1% in MSVF-2 and 83.1% in MSVF-3/m had at least two vertebral fractures in adjacent. The fractured thoracolumbar vertebra in MSVF was less compressed than that in SSVF. Apparent spine trauma was reported by 61.4% of SSVF, 44.1% of MSVF-2, and 36.3% of MSVF-3/m, while early hospitalization with pre-hospital back pain ≤ 1 week was 58.9% in SSVF, 45.3% in MSVF-2, and 25.9% in MSVF-3/m. Only females aged 70-80 years old in MSVF-3/m showed lower baseline bone mineral density than in MSVF-2 and SSVF. MSVF were not associated with increased comorbidity of hypertension, diabetes, coronary heart disease, cerebral infarction, and chronic pulmonary disease.
Conclusions: 20% of acute OVCF can involve multiple vertebra without significant spine trauma or lower baseline bone mineral density. Multiple OVCF tend to occur in adjacent vertebra with less thoracolumbar vertebral compression but longer duration of pre-hospital back pain.
Keywords: Fragility fracture; Multiple fracture; Osteoporosis; Osteoporotic vertebral compression fracture; Vertebral fracture cascades.
© 2023. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Comparison of thoracolumbar versus non-thoracolumbar osteoporotic vertebral compression fractures in risk factors, vertebral compression degree and pre-hospital back pain.J Orthop Surg Res. 2023 Aug 30;18(1):643. doi: 10.1186/s13018-023-04140-6. J Orthop Surg Res. 2023. PMID: 37649026 Free PMC article.
-
Similarities in distribution pattern between acute multiple osteoporotic vertebral compression fractures and vertebral fractures cascades.J Orthop Surg Res. 2024 Dec 19;19(1):844. doi: 10.1186/s13018-024-05337-z. J Orthop Surg Res. 2024. PMID: 39696524 Free PMC article.
-
[Analysis of demographic and clinical characteristics of 744 inpatients with osteoporotic vertebral compression fractures].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025 Mar 15;39(3):354-361. doi: 10.7507/1002-1892.202411068. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025. PMID: 40101912 Free PMC article. Chinese.
-
Correlation analysis of the vertebral compression degree and CT HU value in elderly patients with osteoporotic thoracolumbar fractures.J Orthop Surg Res. 2023 Jun 26;18(1):457. doi: 10.1186/s13018-023-03941-z. J Orthop Surg Res. 2023. PMID: 37365576 Free PMC article. Review.
-
Vertebral compression fractures: Still an unpredictable aspect of osteoporosis.Turk J Med Sci. 2021 Apr 30;51(2):393-399. doi: 10.3906/sag-2005-315. Turk J Med Sci. 2021. PMID: 32967415 Free PMC article. Review.
Cited by
-
Advances in the clinical diagnosis and treatment of multiple-level noncontiguous spinal fractures.Front Neurol. 2024 Nov 21;15:1469425. doi: 10.3389/fneur.2024.1469425. eCollection 2024. Front Neurol. 2024. PMID: 39639988 Free PMC article. Review.
-
The value of quantitative analysis of radionuclide bone SPECT/CT imaging in vertebral compression fracture: a retrospective study.BMC Med Imaging. 2024 Oct 8;24(1):270. doi: 10.1186/s12880-024-01452-9. BMC Med Imaging. 2024. PMID: 39379844 Free PMC article.
-
Thoracolumbar kyphosis prognoses poor results after proximal femoral fracture: a 3-year multicenter prospective cohort study.J Bone Miner Metab. 2025 May;43(3):237-248. doi: 10.1007/s00774-024-01576-6. Epub 2025 Jan 7. J Bone Miner Metab. 2025. PMID: 39777540
-
Factors Influencing the Development of Metachronous Fractures in Patients with Osteoporotic Vertebral Fractures Treated with Conservative Management or Vertebroplasty.Diagnostics (Basel). 2025 Jan 13;15(2):160. doi: 10.3390/diagnostics15020160. Diagnostics (Basel). 2025. PMID: 39857044 Free PMC article.
-
A nomogram for postoperative pain relief in patients with osteoporotic vertebral compression fracture treated with polymethylmethacrylate bone cement.Sci Rep. 2025 Jan 13;15(1):1780. doi: 10.1038/s41598-025-85820-7. Sci Rep. 2025. PMID: 39805925 Free PMC article.
References
-
- Dai C, Liang G, Zhang Y, Dong Y, Zhou X. Risk factors of vertebral re-fracture after PVP or PKP for osteoporotic vertebral compression fractures, especially in Eastern Asia: a systematic review and meta-analysis. J Orthop Surg Res. 2022;17(1):161. doi: 10.1186/s13018-022-03038-z. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
